Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The International Poker RulesДокумент2 страницыThe International Poker RulesOutontheBubbleОценок пока нет
- BIOBASE Vortex Mixer MX-S - MX-F User ManualДокумент10 страницBIOBASE Vortex Mixer MX-S - MX-F User Manualsoporte03Оценок пока нет
- Business Statistic Handout Bba - Sem 2Документ7 страницBusiness Statistic Handout Bba - Sem 2hanirveshОценок пока нет
- PreviewpdfДокумент83 страницыPreviewpdfJohana GavilanesОценок пока нет
- Rare Malignant Glomus Tumor of The Esophagus With PulmonaryДокумент6 страницRare Malignant Glomus Tumor of The Esophagus With PulmonaryRobrigo RexОценок пока нет
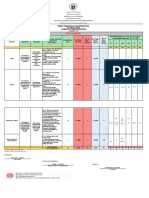
- Revised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10Документ6 страницRevised Final Quarter 1 Tos-Rbt-Sy-2022-2023 Tle-Cookery 10May Ann GuintoОценок пока нет
- Building For The Environment 1Документ3 страницыBuilding For The Environment 1api-133774200Оценок пока нет
- Intervensi Terapi Pada Sepsis PDFДокумент28 страницIntervensi Terapi Pada Sepsis PDFifan zulfantriОценок пока нет
- List of Phrasal Verbs 1 ColumnДокумент12 страницList of Phrasal Verbs 1 ColumnmoiibdОценок пока нет
- Vocations The New Midheaven Extension ProcessДокумент266 страницVocations The New Midheaven Extension ProcessMiss M.100% (24)
- Grade 9 WorkbookДокумент44 страницыGrade 9 WorkbookMaria Russeneth Joy NaloОценок пока нет
- Addition Color by Code: Yellow 1, 2, Blue 3, 4, Pink 5, 6 Peach 7, 8 Light Green 9, 10, Black 11Документ1 страницаAddition Color by Code: Yellow 1, 2, Blue 3, 4, Pink 5, 6 Peach 7, 8 Light Green 9, 10, Black 11Noor NadhirahОценок пока нет
- Applied Physics (PHY-102) Course OutlineДокумент3 страницыApplied Physics (PHY-102) Course OutlineMuhammad RafayОценок пока нет
- Manual Ares-G2 2Документ78 страницManual Ares-G2 2CarolDiasОценок пока нет
- Zahid Imran CVДокумент4 страницыZahid Imran CVDhia Hadj SassiОценок пока нет
- Ac1025 Exc16 (1) .PDFTTTTTTTTTTTTTTTTTTTДокумент50 страницAc1025 Exc16 (1) .PDFTTTTTTTTTTTTTTTTTTTHung Faat ChengОценок пока нет
- N2 V Operare ManualДокумент370 страницN2 V Operare Manualramiro0001Оценок пока нет
- Amp DC, OaДокумент4 страницыAmp DC, OaFantastic KiaОценок пока нет
- The Grass Rink Summer Final 2019Документ9 страницThe Grass Rink Summer Final 2019api-241553699Оценок пока нет
- Standard nfx15-211Документ2 страницыStandard nfx15-211Luis Enrique Cóndor PorrasОценок пока нет
- Meriam Mfc4150 ManДокумент40 страницMeriam Mfc4150 Manwajahatrafiq6607Оценок пока нет
- Bluestar Annual Report 2021-22Документ302 страницыBluestar Annual Report 2021-22Kunal PohaniОценок пока нет
- How To Present A Paper at An Academic Conference: Steve WallaceДокумент122 страницыHow To Present A Paper at An Academic Conference: Steve WallaceJessicaAF2009gmtОценок пока нет
- Lect.1-Investments Background & IssuesДокумент44 страницыLect.1-Investments Background & IssuesAbu BakarОценок пока нет
- NHM Thane Recruitment 2022 For 280 PostsДокумент9 страницNHM Thane Recruitment 2022 For 280 PostsDr.kailas Gaikwad , MO UPHC Turbhe NMMCОценок пока нет
- Benko Gambit-Jacobs and Kinsman, 1999Документ163 страницыBenko Gambit-Jacobs and Kinsman, 1999johnson Greker100% (3)
- Lesson: The Averys Have Been Living in New York Since The Late NinetiesДокумент1 страницаLesson: The Averys Have Been Living in New York Since The Late NinetiesLinea SKDОценок пока нет
- AFAR - 07 - New Version No AnswerДокумент7 страницAFAR - 07 - New Version No AnswerjonasОценок пока нет
- Terminal Blocks: Assembled Terminal Block and SeriesДокумент2 страницыTerminal Blocks: Assembled Terminal Block and SeriesQuan Nguyen TheОценок пока нет
- Feds Subpoena W-B Area Info: He Imes EaderДокумент42 страницыFeds Subpoena W-B Area Info: He Imes EaderThe Times LeaderОценок пока нет