Вам также может понравиться
- Community Assessment Concept MapДокумент1 страницаCommunity Assessment Concept Mapapi-543558169Оценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- An Urgent Response To A Continuing CrisisДокумент48 страницAn Urgent Response To A Continuing CrisisCTV VancouverОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Eo - 018-2021 - Re - Constitution of Badac Auxiliary TeamДокумент3 страницыEo - 018-2021 - Re - Constitution of Badac Auxiliary TeamWest CrameОценок пока нет
- Mmi Study Broken Trust Elders Family FinancesДокумент40 страницMmi Study Broken Trust Elders Family FinancesScott McKayОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Brief History of Heroin UseДокумент24 страницыBrief History of Heroin UsedesmontesОценок пока нет
- Integrated-Case-Plan-Template DTCДокумент5 страницIntegrated-Case-Plan-Template DTClatoyakelly162Оценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Mean, Standard Deviation, Scale, and Verbal Interpretation of Spirituality of The Drug SurrendereesДокумент40 страницMean, Standard Deviation, Scale, and Verbal Interpretation of Spirituality of The Drug SurrendereesNads Lee EnzoОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Intoxicant Enemay of Humanity (English) by Sant Seva Singh Rampur Khera PDFДокумент46 страницIntoxicant Enemay of Humanity (English) by Sant Seva Singh Rampur Khera PDFDr. Kamalroop SinghОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Lifeboat ActivityДокумент7 страницThe Lifeboat Activityrajendiran.sОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- A Social Problem Is A Condition That at Least Some People in A Community View As Being UndesirableДокумент2 страницыA Social Problem Is A Condition That at Least Some People in A Community View As Being UndesirableUma VathyОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Budget of Work Mapeh IVДокумент23 страницыBudget of Work Mapeh IVHaydee Remoluna - Aguilar93% (15)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Special Penal Law RA 9156 (Dangerous Drug Act)Документ48 страницSpecial Penal Law RA 9156 (Dangerous Drug Act)Richard Baker0% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Feminist Review Trust Application FormДокумент8 страницFeminist Review Trust Application FormLeticia GagettiОценок пока нет
- Reviewer 1Документ16 страницReviewer 1Jackylou BlancoОценок пока нет
- Virginia Board of Bar Examiners Character & Fitness QuestionnaireДокумент24 страницыVirginia Board of Bar Examiners Character & Fitness QuestionnaireSusan MiloserОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- APA - DSM 5 Substance Use DisorderДокумент2 страницыAPA - DSM 5 Substance Use DisorderFukha DharmawanОценок пока нет
- Executive Order No. 02 - BadacДокумент5 страницExecutive Order No. 02 - Badackesely esguerraОценок пока нет
- Short Listening Test To Song REHABДокумент1 страницаShort Listening Test To Song REHABBeatriz Esmeralda MartinezОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Pyc4802 Exam 15937224Документ10 страницPyc4802 Exam 15937224LUCRECIA JACOBSОценок пока нет
- Project File00Документ114 страницProject File00Mohammad Junaid KaziОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Module - 5 - Therapeutic ModalitiesДокумент27 страницModule - 5 - Therapeutic ModalitiesKim RodriguezОценок пока нет
- Drug Abuse and Its PreventionДокумент14 страницDrug Abuse and Its PreventionRao Rizwan AliОценок пока нет
- MAPEH 9 Second Quarter - RemedialДокумент13 страницMAPEH 9 Second Quarter - RemedialMELAIDA CASTANAR GARIBAYОценок пока нет
- Parenting Capacity AssessmentsДокумент28 страницParenting Capacity Assessmentsayzlim100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
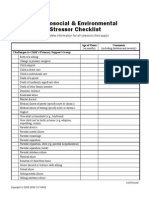
- Mod3 10 Psychosocial and Environmental Stressor ChecklistДокумент3 страницыMod3 10 Psychosocial and Environmental Stressor ChecklisttedescofedericoОценок пока нет
- Drug Abuse QuestionnaireДокумент2 страницыDrug Abuse QuestionnaireLouis NinОценок пока нет
- Ijbepartment of !ebucation: Apr 1 7 Z01ZДокумент18 страницIjbepartment of !ebucation: Apr 1 7 Z01Zmychael14100% (2)
- Substance Related DisordersДокумент28 страницSubstance Related DisordersAlexander HartonoОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- May 2015Документ40 страницMay 2015PROMonthlyОценок пока нет
- Format Conclusion and Recommendation Humss & HeДокумент28 страницFormat Conclusion and Recommendation Humss & HeAriana FiestaОценок пока нет