Вам также может понравиться
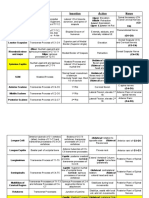
- Muscle Origins, Insertions, Actions, and InterventionsДокумент15 страницMuscle Origins, Insertions, Actions, and InterventionsJoseph Kachelman100% (3)
- NETTER DermatomДокумент1 страницаNETTER Dermatomngwinda90100% (1)
- Lumbosacral PlexusДокумент3 страницыLumbosacral Plexusgehaoi4Оценок пока нет
- Spinal Cord Lesions 1Документ43 страницыSpinal Cord Lesions 1Worthless Boys100% (4)
- (STUART MCGILL - Core Training Evidence Translating To Better PerfoДокумент15 страниц(STUART MCGILL - Core Training Evidence Translating To Better PerfoSakip Hirrim100% (2)
- Spinal Cord ND Spinal NervesДокумент67 страницSpinal Cord ND Spinal NervesfrizkapfОценок пока нет
- Cervical Disc 1Документ68 страницCervical Disc 1Nestor BalboaОценок пока нет
- Anotomy of PNS Irfan AliiДокумент51 страницаAnotomy of PNS Irfan AliiAzeem Ali ShahОценок пока нет
- Structure of A Peripheral NerveДокумент12 страницStructure of A Peripheral NerveFides AdivisoОценок пока нет
- Anatomical LevelsДокумент1 страницаAnatomical LevelspiemaningatОценок пока нет
- Anatomy Systema Nervosum Periphicum Et Autonomicum: Dr. Dodik NursantoДокумент54 страницыAnatomy Systema Nervosum Periphicum Et Autonomicum: Dr. Dodik NursantoDhiastikaОценок пока нет
- Mri Spine by DR ShamolДокумент309 страницMri Spine by DR Shamolالقارئ محمد سيد عباس mohamed sayed abassОценок пока нет
- Lab 5 PNS & Spinal Cord AnswersДокумент12 страницLab 5 PNS & Spinal Cord AnswersCemre KuzeyОценок пока нет
- Back and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsДокумент1 страницаBack and Spinal Cord Study Guide: 2.1 Topographic Anatomy Study AimsMihaelaОценок пока нет
- Brachial Plexus Block: "Dr. Sami Ur Rehman" House OfficerДокумент65 страницBrachial Plexus Block: "Dr. Sami Ur Rehman" House OfficerSami Ur RehmanОценок пока нет
- CH01 Sample PDFДокумент32 страницыCH01 Sample PDFDilah RahmaОценок пока нет
- Description: SKELETAL SYSTEM-Axial SkeletonДокумент18 страницDescription: SKELETAL SYSTEM-Axial SkeletonJessica PalacioОценок пока нет
- EAU Pocket On Neuro Urology 2022Документ13 страницEAU Pocket On Neuro Urology 2022Dane QhОценок пока нет
- MRC Anatomy - Kadakia Final 2019Документ247 страницMRC Anatomy - Kadakia Final 20192qmdjr2qhkОценок пока нет
- Dermatomes+Myotomes Lower Limb Lecture SlidesДокумент13 страницDermatomes+Myotomes Lower Limb Lecture SlidesAnelisiwe DlaminiОценок пока нет
- 00 Neuro Cheat SheetДокумент2 страницы00 Neuro Cheat SheetFranz LibreОценок пока нет
- Dr. AnanyaДокумент55 страницDr. AnanyatarawifaОценок пока нет
- Sci Additional NotesДокумент16 страницSci Additional NotesdescalzotahОценок пока нет
- Anatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomyДокумент53 страницыAnatomy of Brachial Plexus: DR - Sadiq Wadood Siddiqui JR3 Department of AnatomySadiq Wadood SiddiquiОценок пока нет
- Limbs 1b - Overview of Anatomy of Upper and Lower LimbsДокумент5 страницLimbs 1b - Overview of Anatomy of Upper and Lower LimbsTarmizi Md NorОценок пока нет
- Le Plexus BrachialДокумент1 страницаLe Plexus BrachialCarl-Eric TanoéОценок пока нет
- Upper Limb MusclesДокумент1 страницаUpper Limb MusclesVimala ColacoОценок пока нет
- Chapter 4 Sensory and Motor Pathways 2014 Clinical NeuroscienceДокумент11 страницChapter 4 Sensory and Motor Pathways 2014 Clinical NeuroscienceMarta Casals CollОценок пока нет
- Brachial PlexusДокумент72 страницыBrachial PlexusmathivannaninthujanОценок пока нет
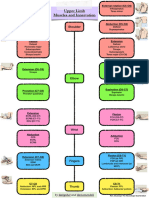
- UPPER LIMB - 6 Spinal Cord Segments, Dermatomes and Myotomes of The Upper LimbДокумент3 страницыUPPER LIMB - 6 Spinal Cord Segments, Dermatomes and Myotomes of The Upper LimbAbbas AliОценок пока нет
- Brachial PlexusДокумент5 страницBrachial PlexusRajveerОценок пока нет
- Dr. Rohmania - Hernia Nukleus PulposusДокумент30 страницDr. Rohmania - Hernia Nukleus PulposusAnonymous FfZm5kOkYFОценок пока нет
- NIOM Anestesi (Autosaved) - 1Документ58 страницNIOM Anestesi (Autosaved) - 1andriruslyОценок пока нет
- How To Draw The Brachial PlexusДокумент16 страницHow To Draw The Brachial PlexusHОценок пока нет
- Pages From (Susan O'Sullivan, Raymond Siegelman) National PhyДокумент1 страницаPages From (Susan O'Sullivan, Raymond Siegelman) National Phydrng48Оценок пока нет
- Muscles of The Superficial BackДокумент3 страницыMuscles of The Superficial BackMargaux Chang NuñezОценок пока нет
- The Brachial Plexus - Sections - Branches - TeachMeAnatomyДокумент10 страницThe Brachial Plexus - Sections - Branches - TeachMeAnatomymohit kumarОценок пока нет
- Back MusclesДокумент1 страницаBack MuscleslrostomeОценок пока нет
- The Brain and Nerves: I I I I I I I I I I IДокумент1 страницаThe Brain and Nerves: I I I I I I I I I I ISALIM BOUAIDОценок пока нет
- Branch of Brachialis PlexusДокумент2 страницыBranch of Brachialis PlexusGrace GozaliОценок пока нет
- Key To Illustration: MUSCULAR SYSTEM-Skeletal MusclesДокумент14 страницKey To Illustration: MUSCULAR SYSTEM-Skeletal MusclesJessica PalacioОценок пока нет
- Brachial PlexusДокумент4 страницыBrachial PlexussaluniasОценок пока нет
- Vertebral Column: Nicole M. Reeves, Ph.D. Department of AnatomyДокумент58 страницVertebral Column: Nicole M. Reeves, Ph.D. Department of Anatomykrishna gОценок пока нет
- Anatomy Supertable With Pics PDFДокумент39 страницAnatomy Supertable With Pics PDFCla NuvalОценок пока нет
- Anatómia ÖsszefoglalóДокумент4 страницыAnatómia ÖsszefoglalóvyolaОценок пока нет
- MSKДокумент7 страницMSKKY KimberlyОценок пока нет
- Ficha OsteowareДокумент2 страницыFicha OsteowarearturosaezОценок пока нет
- Isncsci Worksheet 2015 Web PDFДокумент2 страницыIsncsci Worksheet 2015 Web PDFDavideОценок пока нет
- Dr. Syed Irfan Raza ArifДокумент27 страницDr. Syed Irfan Raza ArifSyed Irfan ArifОценок пока нет
- Nerve Roots and Brancial PlexusДокумент1 страницаNerve Roots and Brancial Plexuscyc9182Оценок пока нет
- And Physiology: The Human AnatomyДокумент14 страницAnd Physiology: The Human AnatomySakshi SharmaОценок пока нет
- 5 Orbit For Dental Students 2Документ18 страниц5 Orbit For Dental Students 2Mohamad TallОценок пока нет
- MMT All MOVEMENTSДокумент3 страницыMMT All MOVEMENTSesha NadeemОценок пока нет
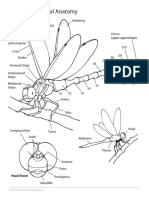
- Dragonfly External AnatomyДокумент1 страницаDragonfly External AnatomyShizzy HeiwajimaОценок пока нет
- Chapter 1 - Overview of The Nervous System - 2014 - Clinical NeuroscienceДокумент17 страницChapter 1 - Overview of The Nervous System - 2014 - Clinical NeuroscienceMarta Casals CollОценок пока нет
- Right Totals (Maximum)Документ6 страницRight Totals (Maximum)kaychi zОценок пока нет
- Ilovepdf Merged MergedДокумент11 страницIlovepdf Merged MergedBbvcbОценок пока нет
- Table of Back Muscles RWДокумент3 страницыTable of Back Muscles RWFrank Zhang100% (1)
- UntitledДокумент59 страницUntitledNidhish K ShettigarОценок пока нет
- Clavicular Head:: RD THДокумент3 страницыClavicular Head:: RD THSam PadreОценок пока нет
- Patient Diagnosis Sheet PDFДокумент1 страницаPatient Diagnosis Sheet PDFNaresh Muttavarapu100% (1)
- BCHDJKДокумент17 страницBCHDJKamelia rahayuОценок пока нет
- Jadwal Ujian Remedial Alih Tahun TAHUN AKADEMIK 2018 - 2019Документ6 страницJadwal Ujian Remedial Alih Tahun TAHUN AKADEMIK 2018 - 2019amelia rahayuОценок пока нет
- Syllabus Laboratory Anatomy Gastrointestinal System: A SequenceДокумент17 страницSyllabus Laboratory Anatomy Gastrointestinal System: A Sequenceamelia rahayuОценок пока нет
- 7985 - Jadwal GIS 1920Документ12 страниц7985 - Jadwal GIS 1920amelia rahayuОценок пока нет
- 9755 - IV Insertion TA 20192020 - WMДокумент2 страницы9755 - IV Insertion TA 20192020 - WMamelia rahayuОценок пока нет
- Laboratory Activity PhysiologyДокумент10 страницLaboratory Activity Physiologyamelia rahayuОценок пока нет
- JhghiДокумент7 страницJhghiamelia rahayuОценок пока нет
- Intra Venous Insertion (Dr. DeddyДокумент2 страницыIntra Venous Insertion (Dr. Deddyamelia rahayuОценок пока нет
- 7985 - Jadwal GIS 1920Документ12 страниц7985 - Jadwal GIS 1920amelia rahayuОценок пока нет
- KKLL WPS OfficeДокумент1 страницаKKLL WPS Officeamelia rahayuОценок пока нет
- Laboratory Activity Physiology: Biomedical Laboratory, Faculty of Medicine, Unisba, Jl. Tamansari No.22 Bandung 40116Документ4 страницыLaboratory Activity Physiology: Biomedical Laboratory, Faculty of Medicine, Unisba, Jl. Tamansari No.22 Bandung 40116amelia rahayuОценок пока нет
- FFF WPS OfficeДокумент1 страницаFFF WPS Officeamelia rahayuОценок пока нет
- Hjnangzhhzhhzh WPS OfficeДокумент1 страницаHjnangzhhzhhzh WPS Officeamelia rahayuОценок пока нет
- BHHJJ WPS OfficeДокумент1 страницаBHHJJ WPS Officeamelia rahayuОценок пока нет
- Superjunior WPS OfficeДокумент1 страницаSuperjunior WPS Officeamelia rahayuОценок пока нет
- RGRDWD WPS OfficeДокумент1 страницаRGRDWD WPS Officeamelia rahayuОценок пока нет
- Apaan WPS OfficeДокумент1 страницаApaan WPS Officeamelia rahayuОценок пока нет
- Amajshb WPS OfficeДокумент1 страницаAmajshb WPS Officeamelia rahayuОценок пока нет
- (Letter Paper) Who Are You-WPS OfficeДокумент1 страница(Letter Paper) Who Are You-WPS Officeamelia rahayuОценок пока нет
- Superjunior WPS OfficeДокумент1 страницаSuperjunior WPS Officeamelia rahayuОценок пока нет
- The Pittston Dispatch 06-05-2011Документ70 страницThe Pittston Dispatch 06-05-2011The Times LeaderОценок пока нет
- New Zealand Acute Low Back Pain GuidelineДокумент70 страницNew Zealand Acute Low Back Pain GuidelineLuis AndradeОценок пока нет
- Labor CA - Ses Batch 3Документ66 страницLabor CA - Ses Batch 3Kring de VeraОценок пока нет
- Mohd Sabri Bin Mohamad Zin V DR M Nachiappan & Anor (20Документ16 страницMohd Sabri Bin Mohamad Zin V DR M Nachiappan & Anor (20hmОценок пока нет
- Differences Between Myelopathy and RadiculopathyДокумент4 страницыDifferences Between Myelopathy and RadiculopathyWidiana KosasihОценок пока нет
- Low Back Pain: Tips On Pain Relief and PreventionДокумент16 страницLow Back Pain: Tips On Pain Relief and PreventionFalcoOonОценок пока нет
- Penatalaksanaan Fisioterapi Pada Dan Mc. Kenzie Exercise Di Rso Prof Dr. R. Soeharso SurakartaДокумент9 страницPenatalaksanaan Fisioterapi Pada Dan Mc. Kenzie Exercise Di Rso Prof Dr. R. Soeharso SurakartaAdy WarsanaОценок пока нет
- Low Back Ache: Capt PramodДокумент67 страницLow Back Ache: Capt PramodPramod MahenderОценок пока нет
- Failure of Endoscopic Spine SurgeryДокумент6 страницFailure of Endoscopic Spine SurgeryKaustubh KeskarОценок пока нет
- (Fitness Sutra Book 1) Chopra, Dr. Monika - Workout For Desk Bounds - Quick Stretches & Exercises To Keep Your Neck, Shoulders, Back & Legs Pain-Free and Mind Active-Fitsutra Wellness PVT LTD (2020)Документ138 страниц(Fitness Sutra Book 1) Chopra, Dr. Monika - Workout For Desk Bounds - Quick Stretches & Exercises To Keep Your Neck, Shoulders, Back & Legs Pain-Free and Mind Active-Fitsutra Wellness PVT LTD (2020)Anh Le100% (2)
- 10 03 11editionДокумент28 страниц10 03 11editionSan Mateo Daily JournalОценок пока нет
- Herniated Nucleus PulposusДокумент29 страницHerniated Nucleus PulposusBanni Aprilita Pratiwi100% (2)
- Facet Joint SyndromeДокумент17 страницFacet Joint Syndromepaulvaso27100% (1)
- Dr. Stephanus Gunawan Sp. BS - IPM or SurgeryДокумент44 страницыDr. Stephanus Gunawan Sp. BS - IPM or SurgeryFreade AkbarОценок пока нет
- Advances in The Diagnosis and Management of Neck PainДокумент19 страницAdvances in The Diagnosis and Management of Neck PainJose Fernando DiezОценок пока нет
- Traction: Cervical & LumbarДокумент21 страницаTraction: Cervical & LumbarBoud ElhassanОценок пока нет
- Risk Factors Forchronic Low Back Pain 2161 0711.1000271Документ4 страницыRisk Factors Forchronic Low Back Pain 2161 0711.100027155664411Оценок пока нет
- Human Spinal Cord Picture C1 To S5 VertebraДокумент3 страницыHuman Spinal Cord Picture C1 To S5 Vertebraajjju02Оценок пока нет
- OMT Evaluation 6Документ34 страницыOMT Evaluation 6aza bellaОценок пока нет
- 14 Surgical Procedures Discectomy and HerniectomyДокумент10 страниц14 Surgical Procedures Discectomy and Herniectomydrkis200Оценок пока нет
- Low Back Pain and Pelvic Girdle Pain in Pregnancy: Review ArticleДокумент11 страницLow Back Pain and Pelvic Girdle Pain in Pregnancy: Review ArticleSaeful RamadonОценок пока нет
- Rathmell2008 2Документ12 страницRathmell2008 2Shaun TylerОценок пока нет
- Neck Hammock v. Does - ComplaintДокумент89 страницNeck Hammock v. Does - ComplaintSarah BursteinОценок пока нет
- Herniated Nucleus Pulposus (HNP)Документ4 страницыHerniated Nucleus Pulposus (HNP)Kevin CamilozaОценок пока нет
- Cervical Herniated Disc or Ruptured DiscДокумент4 страницыCervical Herniated Disc or Ruptured DiscUwais AlОценок пока нет
- JOSPT Anthony Delitto (2012)Документ57 страницJOSPT Anthony Delitto (2012)Bruno RechОценок пока нет
- Lumbar Facet Pain ArticleДокумент24 страницыLumbar Facet Pain ArticlejmccoyОценок пока нет