Вам также может понравиться
- User's GuideДокумент51 страницаUser's GuiderisyadanangОценок пока нет
- Consensus Term For Central Neck DissectionДокумент9 страницConsensus Term For Central Neck DissectionStanley ProbosenoОценок пока нет
- Tumor MarkerДокумент19 страницTumor MarkerStanley ProbosenoОценок пока нет
- Cancer Epidemiology in Older Adolescents & Young Adult 15-29 Years of AgeДокумент218 страницCancer Epidemiology in Older Adolescents & Young Adult 15-29 Years of AgeStanley ProbosenoОценок пока нет
- Thyroid and PregnancyДокумент2 страницыThyroid and PregnancyStanley ProbosenoОценок пока нет
- Thyroid and PregnancyДокумент2 страницыThyroid and PregnancyStanley ProbosenoОценок пока нет
- Well Differentiated Thyroid CancerДокумент11 страницWell Differentiated Thyroid CancerStanley ProbosenoОценок пока нет
- Management of Childhood ITPДокумент5 страницManagement of Childhood ITPStanley ProbosenoОценок пока нет
- 6th Central Pay Commission Salary CalculatorДокумент15 страниц6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Goodenough Draw A PersonДокумент2 страницыGoodenough Draw A PersonChoky Chokie ChocoОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Date Company Code Bank RefДокумент16 страницDate Company Code Bank RefSrinivas YОценок пока нет
- ASTM 210cДокумент1 страницаASTM 210cDodi SuhendraОценок пока нет
- 0100CT1901 Sec-23 102520202Документ120 страниц0100CT1901 Sec-23 102520202Chandra SekaranОценок пока нет
- RRB Group DДокумент35 страницRRB Group DRITESH KUMARОценок пока нет
- User's Manual Installation Guide for Wind DisplayДокумент21 страницаUser's Manual Installation Guide for Wind DisplayVM ServicesОценок пока нет
- Ludwig Von Bertalanffy-General System Theory-Braziller (1968) PDFДокумент153 страницыLudwig Von Bertalanffy-General System Theory-Braziller (1968) PDFM_Eddie0% (1)
- Ax2012 Enus Sam 04 PDFДокумент26 страницAx2012 Enus Sam 04 PDFErnesto J DuranОценок пока нет
- Installation - Operation - Maintenance - Instructions - 30 HXC PDFДокумент36 страницInstallation - Operation - Maintenance - Instructions - 30 HXC PDFNurmansyah Dwi Cahyono100% (3)
- The Contemporary WorldДокумент9 страницThe Contemporary WorldDennis RaymundoОценок пока нет
- Managing Operations AssignmentДокумент17 страницManaging Operations AssignmentNaidu01100% (1)
- Definitions of CEC2017 Benchmark Suite Final Version UpdatedДокумент34 страницыDefinitions of CEC2017 Benchmark Suite Final Version Updatedpc100% (1)
- Product Specification: Part Name: OEL Display Module Part ID: UG-2864HSWEG01 Doc No.: SAS1-9046Документ30 страницProduct Specification: Part Name: OEL Display Module Part ID: UG-2864HSWEG01 Doc No.: SAS1-9046mariОценок пока нет
- Videojet 3140: Laser Marking SystemДокумент2 страницыVideojet 3140: Laser Marking SystemSudiptoОценок пока нет
- KANSAS CITY Hyatt Regency Hotel Walkways CollapseДокумент8 страницKANSAS CITY Hyatt Regency Hotel Walkways CollapseRafran RoslyОценок пока нет
- How To Read Architect DrawingДокумент32 страницыHow To Read Architect DrawingKutty Mansoor50% (2)
- Cisco CCIE CCNP RS Study Flashcards Ver 49Документ102 страницыCisco CCIE CCNP RS Study Flashcards Ver 49niboozОценок пока нет
- Citrix Xen Desktop Interview Questions and Answers - Citrix Xen Desktop FAQsДокумент3 страницыCitrix Xen Desktop Interview Questions and Answers - Citrix Xen Desktop FAQsAnonymous rNmxZViYaОценок пока нет
- OTC13998Документ15 страницOTC13998Raifel MoralesОценок пока нет
- EZSkin v3 User GuideДокумент16 страницEZSkin v3 User GuidePg1978Оценок пока нет
- Dekut Teaching Practice ManualДокумент20 страницDekut Teaching Practice Manualstephen njorogeОценок пока нет
- Binary PDFДокумент13 страницBinary PDFbyprasadОценок пока нет
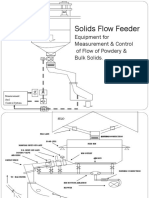
- Solids Flow Feeder Equipment for Precise Measurement & ControlДокумент7 страницSolids Flow Feeder Equipment for Precise Measurement & ControlAbhishek DuttaОценок пока нет
- Sevice Manual BOBCAT S630 PDFДокумент890 страницSevice Manual BOBCAT S630 PDFArtemio Garcia Barrientos100% (11)
- Nitya Parayana Slokas MalayalamДокумент3 страницыNitya Parayana Slokas MalayalamGopakumar NairОценок пока нет
- Mindmup Group-2Документ10 страницMindmup Group-2api-271772521Оценок пока нет
- MMDS Indoor/Outdoor Transmitter Manual: Chengdu Tengyue Electronics Co., LTDДокумент6 страницMMDS Indoor/Outdoor Transmitter Manual: Chengdu Tengyue Electronics Co., LTDHenry Jose OlavarrietaОценок пока нет
- Pyxis SPT HepДокумент597 страницPyxis SPT HepanithaarumallaОценок пока нет
- Project Management Book PDFДокумент55 страницProject Management Book PDFSerigne Mbaye Diop94% (16)
- PBV20N2 Service Manual PDFДокумент244 страницыPBV20N2 Service Manual PDFJack Norhy100% (1)