Вам также может понравиться
- The Secret Language of AttractionДокумент278 страницThe Secret Language of Attractionsandrojairdhonre89% (93)
- Tower Light Inspection ChecklistДокумент19 страницTower Light Inspection ChecklistMOHAMMED RIYAN TОценок пока нет
- Anatomy 090819Документ30 страницAnatomy 090819Vaishnavi GourabathiniОценок пока нет
- Effect of Prepregnancy Body Mass Index and Gestational Weight Gain On Obstetric and Neonatal Outcomes - A Pilot StudyДокумент5 страницEffect of Prepregnancy Body Mass Index and Gestational Weight Gain On Obstetric and Neonatal Outcomes - A Pilot StudyJubair NewazОценок пока нет
- BDI Scores and Risk of Breast Disease and CancerДокумент6 страницBDI Scores and Risk of Breast Disease and CancerRenz MacionОценок пока нет
- Ofir 2003Документ5 страницOfir 2003Jim HawkinsОценок пока нет
- Obesity in PregnancyДокумент13 страницObesity in PregnancynurulmhidayatОценок пока нет
- Relationship Between Low Maternal Vitamin D Status and The Risk of Severe Preeclampsia: A Case Control StudyДокумент10 страницRelationship Between Low Maternal Vitamin D Status and The Risk of Severe Preeclampsia: A Case Control StudyCindy DelapazОценок пока нет
- Prevalence and Determinants of Low Birth Weight: A Case-Con-trol Study in Marrakesh (Morocco)Документ3 страницыPrevalence and Determinants of Low Birth Weight: A Case-Con-trol Study in Marrakesh (Morocco)Michael JonesОценок пока нет
- Pengaruh Kelebihan Berat Badan Ibu, Obesitas Dan Berat Badan Kehamilan Pada Hasil Perinatal Pada Wanita Dengan Diabetes MellitusДокумент8 страницPengaruh Kelebihan Berat Badan Ibu, Obesitas Dan Berat Badan Kehamilan Pada Hasil Perinatal Pada Wanita Dengan Diabetes Mellitusshabrina KdgОценок пока нет
- CHSJ 47 04 10 2021Документ6 страницCHSJ 47 04 10 2021mihail.boldeanuОценок пока нет
- Memahami Usg PDFДокумент8 страницMemahami Usg PDFtasirohОценок пока нет
- Examining The Associations Among Fibrocystic Breast Change, Total Lean Mass, and Percent Body FatДокумент6 страницExamining The Associations Among Fibrocystic Breast Change, Total Lean Mass, and Percent Body FatMichiko MeritasariОценок пока нет
- Risk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalДокумент7 страницRisk Factors of Cesarean Delivery Due To Cephalopelvic Disproportion in Nulliparous Women at Sisaket HospitalManangioma ManОценок пока нет
- Original ArticleДокумент7 страницOriginal ArticleManar ShamielhОценок пока нет
- 159 757 2 PBДокумент6 страниц159 757 2 PBmeldhaОценок пока нет
- Poster Konika NPM ReДокумент1 страницаPoster Konika NPM ReAhmad IsmatullahОценок пока нет
- Obesidad en El EmbarazoДокумент17 страницObesidad en El Embarazodianaarias1703Оценок пока нет
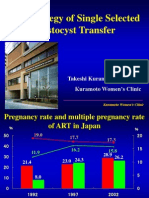
- The Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicДокумент43 страницыThe Strategy of Single Selected Blastocyst Transfer: Takeshi Kuramoto MD, PHD Kuramoto Women'S ClinicDian Isti AngrainiОценок пока нет
- A Descriptive Study To Assess The Morbidity Pattern Among Nurses With Special Reference To ObesityДокумент9 страницA Descriptive Study To Assess The Morbidity Pattern Among Nurses With Special Reference To ObesityEditor IJTSRDОценок пока нет
- Predict LBW with fundal height chartsДокумент4 страницыPredict LBW with fundal height chartsanu snehaОценок пока нет
- 1238 8440 1 PBДокумент6 страниц1238 8440 1 PBKriti KumariОценок пока нет
- PIIS1472648311004226Документ19 страницPIIS1472648311004226Corinne PeanОценок пока нет
- Obesity in Pregnancy review articleДокумент12 страницObesity in Pregnancy review articleClaudia AlessandraОценок пока нет
- Pregnant Women With Morbid Obesity: Pregnancy and Perinatal OutcomesДокумент6 страницPregnant Women With Morbid Obesity: Pregnancy and Perinatal OutcomesVince Daniel VillalbaОценок пока нет
- Magro-Malosso Et Al-2017-Acta Obstetricia Et Gynecologica ScandinavicaДокумент11 страницMagro-Malosso Et Al-2017-Acta Obstetricia Et Gynecologica ScandinavicaRisnaAyhuОценок пока нет
- Project FafaДокумент48 страницProject Fafafarzana abdullahОценок пока нет
- Maternal and Perinatal Outcome of Maternal Obesity atДокумент6 страницMaternal and Perinatal Outcome of Maternal Obesity attaufik perdanaОценок пока нет
- Iajt 00 I 4 P 156Документ5 страницIajt 00 I 4 P 156api-3702148Оценок пока нет
- Obstetrics Outcomes of Pregnancy With Uterine Fibroids in Tertiary Care HospitalДокумент4 страницыObstetrics Outcomes of Pregnancy With Uterine Fibroids in Tertiary Care HospitalMohan Kumar DОценок пока нет
- Childbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyДокумент54 страницыChildbirth and The Female Pelvic Floor: Christopher Maher Wesley UrogynaecologyVeronica MendozaОценок пока нет
- D'Souza-2019-Maternal Body Mass Index and PregДокумент17 страницD'Souza-2019-Maternal Body Mass Index and PregMARIATUL QIFTIYAHОценок пока нет
- Eclampsia: An Enigma: Chitra JoshiДокумент4 страницыEclampsia: An Enigma: Chitra JoshiM Haris Yoga IswantoroОценок пока нет
- Utilization of Postnatal Care Services at Timagi Health Center Three, Oyam DistrictДокумент11 страницUtilization of Postnatal Care Services at Timagi Health Center Three, Oyam DistrictKIU PUBLICATION AND EXTENSIONОценок пока нет
- Risk Factors and Clinical Characteristics of Recurrent Ectopic Pregnancy: A Case - Control StudyДокумент6 страницRisk Factors and Clinical Characteristics of Recurrent Ectopic Pregnancy: A Case - Control StudyYogi ImamОценок пока нет
- Compare The Histological Features Between The Normal and Hypertensive PlacentaДокумент7 страницCompare The Histological Features Between The Normal and Hypertensive PlacentaKamran AmeerОценок пока нет
- Effect of Body Mass Index On Intrauterine Insemination Cycle SuccessДокумент8 страницEffect of Body Mass Index On Intrauterine Insemination Cycle SuccessCarlos ParraОценок пока нет
- Mullin 2002Документ6 страницMullin 2002Khairun NisaОценок пока нет
- Risk Factors For Pelvic Surgery: Y.E. Erata B. Kilic S. Güçlü U. Saygili T. UsluДокумент5 страницRisk Factors For Pelvic Surgery: Y.E. Erata B. Kilic S. Güçlü U. Saygili T. UsluGleiciane AguiarОценок пока нет
- Maternal and Perinatal Outcome of Maternal Obesity atДокумент7 страницMaternal and Perinatal Outcome of Maternal Obesity atappОценок пока нет
- J Ajog 2019 05 022Документ17 страницJ Ajog 2019 05 022DWI LESTARIОценок пока нет
- Gestational DiabetesДокумент1 страницаGestational DiabetesPovilas VarnelisОценок пока нет
- BMI in PregnancyДокумент4 страницыBMI in PregnancyCitra KristiОценок пока нет
- Symphysis-Fundal Height and Abdominal Circumference Measurements As Indicators For Birth WeightДокумент8 страницSymphysis-Fundal Height and Abdominal Circumference Measurements As Indicators For Birth Weighttangam sharmaОценок пока нет
- A Study of Intrauterine Fetal Death in A Tertiary Care HospitalДокумент4 страницыA Study of Intrauterine Fetal Death in A Tertiary Care HospitalintanОценок пока нет
- The Success of Post-Placental Intra-Uterine Device (IUD) at Simo Public HospitalДокумент5 страницThe Success of Post-Placental Intra-Uterine Device (IUD) at Simo Public HospitalAnonymous UHnQSkxLBDОценок пока нет
- Evaluation of Postpartum Female Sterilizations: A Retrospective Study at Tertiary Care Hospital in JammuДокумент6 страницEvaluation of Postpartum Female Sterilizations: A Retrospective Study at Tertiary Care Hospital in JammuIJAR JOURNALОценок пока нет
- Risk Factors For Breast Cancer in Iranian Women Aged Less Than 40yearsДокумент3 страницыRisk Factors For Breast Cancer in Iranian Women Aged Less Than 40yearsMuhammad RobyОценок пока нет
- Ojsadmin, 197Документ4 страницыOjsadmin, 197Theo MendeleyОценок пока нет
- Efektivitas Pemberian Air Kelapa Hijau (Cocos Nucifera L) Untuk Mengatasi DismenoreДокумент7 страницEfektivitas Pemberian Air Kelapa Hijau (Cocos Nucifera L) Untuk Mengatasi DismenoreAdrilia AnissaОценок пока нет
- Meconium-Stained Amniotic Fluid and Meconium Aspiration Syndrome: A Prospective StudyДокумент6 страницMeconium-Stained Amniotic Fluid and Meconium Aspiration Syndrome: A Prospective StudyGem EleanorОценок пока нет
- The Incidence and Complications of Teenage Pregnancy at Chonburi HospitalДокумент6 страницThe Incidence and Complications of Teenage Pregnancy at Chonburi Hospitaledi khoirumanОценок пока нет
- Body Image: Viren Swami, Adrian FurnhamДокумент6 страницBody Image: Viren Swami, Adrian FurnhamNiken DwiОценок пока нет
- DEMOUCHE 2019 Environmental Factors and Risk of Prematurity in West AlgeriaДокумент8 страницDEMOUCHE 2019 Environmental Factors and Risk of Prematurity in West AlgeriaMELALIH AhmedОценок пока нет
- Effect of Birth Weight On Adverse Obstetric.20 PDFДокумент6 страницEffect of Birth Weight On Adverse Obstetric.20 PDFTriponiaОценок пока нет
- Epidemiology of Stillbirth in Rural IndiaДокумент4 страницыEpidemiology of Stillbirth in Rural IndiaArun MorayОценок пока нет
- Incidence and Correlates of Preterm Birth at Hoima Regional Referral HospitalДокумент8 страницIncidence and Correlates of Preterm Birth at Hoima Regional Referral HospitalKIU PUBLICATION AND EXTENSIONОценок пока нет
- The Relationship Between Body Mass Index and Menarche in Adolescents in OwerriДокумент6 страницThe Relationship Between Body Mass Index and Menarche in Adolescents in Owerriijmb333Оценок пока нет
- Jurnal PTB-feritinДокумент4 страницыJurnal PTB-feritindewi wahyuniОценок пока нет
- Childhood Obesity in Iraq: Prevalence and Possible Risk FactorsДокумент5 страницChildhood Obesity in Iraq: Prevalence and Possible Risk FactorsAli AlhamdaniОценок пока нет
- Effect of Delayed Obstetric Labor Care During The COVID 19 Pandemic On Perinatal OutcomesДокумент3 страницыEffect of Delayed Obstetric Labor Care During The COVID 19 Pandemic On Perinatal OutcomesAngela SaldajenoОценок пока нет
- Living with Metastatic Breast Cancer: Stories of Faith and HopeОт EverandLiving with Metastatic Breast Cancer: Stories of Faith and HopeОценок пока нет
- Hormone Therapy: Current Drugs for Treating Breast Cancer – What You Must KnowОт EverandHormone Therapy: Current Drugs for Treating Breast Cancer – What You Must KnowРейтинг: 5 из 5 звезд5/5 (1)
- 698 2956 1 PBДокумент4 страницы698 2956 1 PBimeldafitriОценок пока нет
- Journal of Neonatal Nursing: ReviewДокумент6 страницJournal of Neonatal Nursing: ReviewimeldafitriОценок пока нет
- Crackers Enhanced with Striped Catfish and Carrot FlourДокумент8 страницCrackers Enhanced with Striped Catfish and Carrot FlourimeldafitriОценок пока нет
- Lampiran 3 Form Semi Quantitative Food Frequency Questionnaire (SQ-FFQ)Документ5 страницLampiran 3 Form Semi Quantitative Food Frequency Questionnaire (SQ-FFQ)imeldafitriОценок пока нет
- Parasitologi Kebidanan: Edition Lea & Febiger Philadelphia 1984Документ3 страницыParasitologi Kebidanan: Edition Lea & Febiger Philadelphia 1984imeldafitriОценок пока нет
- 78 Djoko Kartono - Sosialisasi AKGДокумент22 страницы78 Djoko Kartono - Sosialisasi AKGimeldafitriОценок пока нет
- 79-Article Text-330-1-10-20181022Документ13 страниц79-Article Text-330-1-10-20181022imeldafitriОценок пока нет
- CPNS Kemenkes 2019Документ38 страницCPNS Kemenkes 2019imeldafitriОценок пока нет
- 383 Leiyla Elvizahro G2C007043Документ46 страниц383 Leiyla Elvizahro G2C007043Herlambang Cahyo NОценок пока нет
- 383 Leiyla Elvizahro G2C007043Документ46 страниц383 Leiyla Elvizahro G2C007043Herlambang Cahyo NОценок пока нет
- Implementasi Program Keluarga Sadar Gizi (Kadarzi) Di Kabupaten SemarangДокумент10 страницImplementasi Program Keluarga Sadar Gizi (Kadarzi) Di Kabupaten SemarangimeldafitriОценок пока нет
- Ikan Patin PDFДокумент9 страницIkan Patin PDFimeldafitriОценок пока нет
- Pregnancy Weight Gain and Birth OutcomesДокумент10 страницPregnancy Weight Gain and Birth OutcomesimeldafitriОценок пока нет
- Article1385135472 - Rezaie Et AlДокумент5 страницArticle1385135472 - Rezaie Et AlimeldafitriОценок пока нет
- PDFДокумент5 страницPDFimeldafitriОценок пока нет
- 78 Djoko Kartono - Sosialisasi AKGДокумент22 страницы78 Djoko Kartono - Sosialisasi AKGimeldafitriОценок пока нет
- International Journal of Health Sciences and Research: Maternal Nutritional Status and Its Relation With Birth WeightДокумент12 страницInternational Journal of Health Sciences and Research: Maternal Nutritional Status and Its Relation With Birth WeightimeldafitriОценок пока нет
- Energy and Protein Intake in Pregnancy (Review) : Kramer MS, Kakuma RДокумент84 страницыEnergy and Protein Intake in Pregnancy (Review) : Kramer MS, Kakuma RimeldafitriОценок пока нет
- 10 5530ijopp 10 1 5 PDFДокумент6 страниц10 5530ijopp 10 1 5 PDFimeldafitriОценок пока нет
- International Journal of Health Sciences and Research: Maternal Nutritional Status and Its Relation With Birth WeightДокумент12 страницInternational Journal of Health Sciences and Research: Maternal Nutritional Status and Its Relation With Birth WeightimeldafitriОценок пока нет
- The SOAP Note FormatДокумент8 страницThe SOAP Note Formatimeldafitri100% (1)
- 10 5530ijopp 10 1 5 PDFДокумент6 страниц10 5530ijopp 10 1 5 PDFimeldafitriОценок пока нет
- Dok SydneyДокумент8 страницDok SydneyimeldafitriОценок пока нет
- 10 5530ijopp 10 1 5 PDFДокумент6 страниц10 5530ijopp 10 1 5 PDFimeldafitriОценок пока нет
- Midwifery Care Process FinalДокумент3 страницыMidwifery Care Process FinalNico Pieter100% (6)
- The Effects of Oral Contraceptives On Detection and Pain Thresholds As Well As Headache Intensity During Menstrual Cycle in MigraineДокумент13 страницThe Effects of Oral Contraceptives On Detection and Pain Thresholds As Well As Headache Intensity During Menstrual Cycle in MigraineimeldafitriОценок пока нет
- Carbs - Good, Bad and WholegrainДокумент4 страницыCarbs - Good, Bad and WholegrainimeldafitriОценок пока нет
- PDFДокумент8 страницPDFimeldafitriОценок пока нет
- Perbandingan Kadar Protein Dan Lemak Dalam ASI "X", Susu Sapi Formula "Y" Dan Susu Kedelai Formula "Z"Документ13 страницPerbandingan Kadar Protein Dan Lemak Dalam ASI "X", Susu Sapi Formula "Y" Dan Susu Kedelai Formula "Z"Karne AprillianyОценок пока нет
- GuideДокумент2 страницыGuideMaissyОценок пока нет
- Magnets Catalog 2001Документ20 страницMagnets Catalog 2001geckx100% (2)
- Chams 1Документ78 страницChams 1Das RavindraОценок пока нет
- Socio-cultural influences on educationДокумент4 страницыSocio-cultural influences on educationofelia acostaОценок пока нет
- Asus X553MA Repair Guide Rev2.0Документ7 страницAsus X553MA Repair Guide Rev2.0UMA AKANDU UCHEОценок пока нет
- Symasym BBДокумент37 страницSymasym BBChandraRizkyОценок пока нет
- Effect of Dust On The Performance of Wind Turbines PDFДокумент12 страницEffect of Dust On The Performance of Wind Turbines PDFJallal ArramachОценок пока нет
- Administrations whose CoCs are accepted for CECДокумент1 страницаAdministrations whose CoCs are accepted for CECGonçalo CruzeiroОценок пока нет
- Assignment 2Документ4 страницыAssignment 2maxamed0% (1)
- IonosondeДокумент3 страницыIonosondeFaizan GoharОценок пока нет
- EDIBLE VACCINES: A COST-EFFECTIVE SOLUTIONДокумент21 страницаEDIBLE VACCINES: A COST-EFFECTIVE SOLUTIONPritish SareenОценок пока нет
- Litz Wire Termination GuideДокумент5 страницLitz Wire Termination GuideBenjamin DoverОценок пока нет
- TelanganaДокумент16 страницTelanganaRamu Palvai0% (1)
- Technology & Livelihood Education: WEEK 6-7Документ28 страницTechnology & Livelihood Education: WEEK 6-7my musicОценок пока нет
- Turabian Sample PaperДокумент9 страницTurabian Sample Paperemme_lopez908133% (3)
- RA 5921 and RA 10918Документ32 страницыRA 5921 and RA 10918Hani Loveres100% (1)
- GEHC DICOM Conformance CentricityRadiologyRA600 V6 1 DCM 1030 001 Rev6 1 1Документ73 страницыGEHC DICOM Conformance CentricityRadiologyRA600 V6 1 DCM 1030 001 Rev6 1 1mrzdravko15Оценок пока нет
- Graphic Organizers for Organizing IdeasДокумент11 страницGraphic Organizers for Organizing IdeasMargie Tirado JavierОценок пока нет
- 03 Seatwork 1 ProjectManagement SenisRachelДокумент2 страницы03 Seatwork 1 ProjectManagement SenisRachelRachel SenisОценок пока нет
- SAP SD Course Content PDFДокумент4 страницыSAP SD Course Content PDFshuku03Оценок пока нет
- Academic Writing & IdentityДокумент218 страницAcademic Writing & IdentityGustavo RegesОценок пока нет
- Acid content in fruitsДокумент2 страницыAcid content in fruitsbone fire100% (1)
- Process of Producting High Carbon Ferro ChromeДокумент5 страницProcess of Producting High Carbon Ferro ChromeSantosh Kumar MahtoОценок пока нет
- English For Academic Purposes (EAP) : Lecture 5: Past SimpleДокумент11 страницEnglish For Academic Purposes (EAP) : Lecture 5: Past Simplealmastar officeОценок пока нет
- Sight Reduction Tables For Marine Navigation: B, R - D, D. SДокумент12 страницSight Reduction Tables For Marine Navigation: B, R - D, D. SGeani MihaiОценок пока нет
- ANAPHYДокумент23 страницыANAPHYYu, Denise Kyla BernadetteОценок пока нет
- New Company Profile.Документ8 страницNew Company Profile.Allen AsirОценок пока нет