Вам также может понравиться
- Episode 6: Deductive and Inductive Methods of Teaching: My Learning Episode OverviewДокумент10 страницEpisode 6: Deductive and Inductive Methods of Teaching: My Learning Episode OverviewJustine Elle Vijar85% (13)
- Iop HT 7Документ9 страницIop HT 7Peer TutorОценок пока нет
- Role of Hypertension As A Risk Factor OAGДокумент9 страницRole of Hypertension As A Risk Factor OAGAndhika PutraОценок пока нет
- Prospective Study of Fasting Blood Glucose and Intracerebral Hemorrhagic RiskДокумент7 страницProspective Study of Fasting Blood Glucose and Intracerebral Hemorrhagic Riskhidayatul rahmoОценок пока нет
- Chest: Postgraduate Education CornerДокумент10 страницChest: Postgraduate Education Cornerdimas adjie pangestuОценок пока нет
- Hypertensionaha 118 11819-2Документ2 страницыHypertensionaha 118 11819-2Sari RakhmawatiОценок пока нет
- What Is NTGДокумент4 страницыWhat Is NTGSonia RogersОценок пока нет
- Bjophthalmol 2018 311897.fullДокумент8 страницBjophthalmol 2018 311897.fullKrisnaОценок пока нет
- I1552 5783 60 14 4548 PDFДокумент8 страницI1552 5783 60 14 4548 PDFNetflix DheaОценок пока нет
- Accepted Manuscript: YprrvДокумент27 страницAccepted Manuscript: YprrvTiara Grhanesia DenashuryaОценок пока нет
- Ibyt 13 I 4 P 659Документ10 страницIbyt 13 I 4 P 659Sadhira GitaОценок пока нет
- Current Incidence and Outcome of The Acute Respiratory Distress SyndromeДокумент6 страницCurrent Incidence and Outcome of The Acute Respiratory Distress Syndromedarius2311Оценок пока нет
- CKD HT 3Документ8 страницCKD HT 3Peer TutorОценок пока нет
- Heart Volume Issue 2017 (Doi 10.1136 - Heartjnl-2017-312112) Ruwald, Martin H - Syncope andДокумент3 страницыHeart Volume Issue 2017 (Doi 10.1136 - Heartjnl-2017-312112) Ruwald, Martin H - Syncope andZauzaОценок пока нет
- Anemia in Heart FailureДокумент8 страницAnemia in Heart FailuremardianrnОценок пока нет
- Dci 210017Документ3 страницыDci 210017Gloria WuОценок пока нет
- A Correlational Study of Systemic Blood Pressure and IOP HL SITHOLEДокумент6 страницA Correlational Study of Systemic Blood Pressure and IOP HL SITHOLESurya Nirmala DewiОценок пока нет
- Primary Aldosteronism, Aldosterone, and Extracellular VesiclesДокумент9 страницPrimary Aldosteronism, Aldosterone, and Extracellular VesiclesYo MeОценок пока нет
- E001559 FullДокумент10 страницE001559 FullMohammad Chandra dwi pОценок пока нет
- Hypertensionaha 108 190329 PDFДокумент19 страницHypertensionaha 108 190329 PDFRJ CabaОценок пока нет
- Pulmonary Arterial Hypertension in Infants With Chronic Lung Disease: Will We Ever Understand It?Документ5 страницPulmonary Arterial Hypertension in Infants With Chronic Lung Disease: Will We Ever Understand It?Adrian KhomanОценок пока нет
- Barst RJ 2011 Pulmonary Arterial Hypertension A Comparison Between Children and AdultsДокумент13 страницBarst RJ 2011 Pulmonary Arterial Hypertension A Comparison Between Children and Adultsdr.herusetiawanОценок пока нет
- HHS Public Access: Pulmonary Hypertension in ChildrenДокумент44 страницыHHS Public Access: Pulmonary Hypertension in ChildrenLina María CañónОценок пока нет
- International Journal of Pharma and Bio Sciences: BiochemistryДокумент5 страницInternational Journal of Pharma and Bio Sciences: BiochemistryAkbar LimpoОценок пока нет
- Kent, Et Al. 2020 - StrokeДокумент5 страницKent, Et Al. 2020 - StrokeCARLOS SANTIAGO PEREZ RODRIGUEZОценок пока нет
- Chadsvasc and HasbledДокумент4 страницыChadsvasc and HasbledPGI AnaesthesiaОценок пока нет
- Oxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaДокумент9 страницOxidative Stress and Lipid Profile Among Hypertensive Patients at A Tertiary Centre in Kano, Northwest, NigeriaidiОценок пока нет
- Chest: Cardiovascular Comorbidity in COPDДокумент16 страницChest: Cardiovascular Comorbidity in COPDAndry Wahyudi AgusОценок пока нет
- Hypertensive Disorders of Pregnancy and Long-Term Risk of Maternal Stroke-A Systematic Review and Meta-AnalysisДокумент21 страницаHypertensive Disorders of Pregnancy and Long-Term Risk of Maternal Stroke-A Systematic Review and Meta-AnalysisprofnutrialecuriОценок пока нет
- Control of Hypertension and Risk of Stroke Recurrence: Gary Friday, MD, MPH Milton Alter, MD, PHD Sue-Min Lai, PHD, MsДокумент7 страницControl of Hypertension and Risk of Stroke Recurrence: Gary Friday, MD, MPH Milton Alter, MD, PHD Sue-Min Lai, PHD, MsDeudeu Durotun NafisahОценок пока нет
- Traducir NeurologiaДокумент23 страницыTraducir Neurologiaclara aquino mayangaОценок пока нет
- The Journal For Nurse Practitioners: Jacqueline O'Toole, MSC, NP, Irene Gibson, Ma, RGN, Gerard T. Flaherty, MDДокумент4 страницыThe Journal For Nurse Practitioners: Jacqueline O'Toole, MSC, NP, Irene Gibson, Ma, RGN, Gerard T. Flaherty, MDGina GuisamanoОценок пока нет
- 2001 Relationship of Blood Pressure To 25-Year Mortality Due To Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult MenДокумент8 страниц2001 Relationship of Blood Pressure To 25-Year Mortality Due To Coronary Heart Disease, Cardiovascular Diseases, and All Causes in Young Adult MencarlosОценок пока нет
- Prognostic Factors in Pulmonary Arterial Hypertension: Literature ReviewДокумент5 страницPrognostic Factors in Pulmonary Arterial Hypertension: Literature Reviewhuda riyambodoОценок пока нет
- Hajiaghajani 2021Документ13 страницHajiaghajani 2021Camilo HernándezОценок пока нет
- Blood Pressure and OxygenationДокумент7 страницBlood Pressure and OxygenationRoberto ZelayaОценок пока нет
- Prognostic Value of Admission Blood Glucose in Diabetic and Non-Diabetic Patients With Intracerebral HemorrhageДокумент7 страницPrognostic Value of Admission Blood Glucose in Diabetic and Non-Diabetic Patients With Intracerebral HemorrhageNur Irma SafitriОценок пока нет
- Sleep and HypertensionДокумент10 страницSleep and HypertensionPutraОценок пока нет
- Obstructive Sleep Apnoea Syndrome As A Risk Factor For Hypertension: Population StudyДокумент4 страницыObstructive Sleep Apnoea Syndrome As A Risk Factor For Hypertension: Population StudyNelson OlivarОценок пока нет
- Anemia in Heart Failure: Still Relevant?Документ8 страницAnemia in Heart Failure: Still Relevant?Hedya Nadhrati SururaОценок пока нет
- Postgradmedj 96 525Документ5 страницPostgradmedj 96 525Huda TrisenaОценок пока нет
- Latest Strategy in Renal Anemia Management in Peritoneal Dialysis PatientsДокумент5 страницLatest Strategy in Renal Anemia Management in Peritoneal Dialysis PatientsMamad TrihatmowidjoyoОценок пока нет
- Mapaennios Aha Hypertension2008Документ20 страницMapaennios Aha Hypertension2008Mr. ShadenfreudeОценок пока нет
- Pubmed 3Документ11 страницPubmed 3Adam PrabataОценок пока нет
- Chronicsubdural Hematoma: Epidemiology and Natural HistoryДокумент6 страницChronicsubdural Hematoma: Epidemiology and Natural HistoryalgoОценок пока нет
- NeldamДокумент10 страницNeldamdini hanifaОценок пока нет
- Dose-Response Association Between Physical Activity and Incident HypertensionДокумент8 страницDose-Response Association Between Physical Activity and Incident HypertensionRirin Van GobelОценок пока нет
- NTG Practical ApproachДокумент6 страницNTG Practical ApproachRasha Mounir Abdel-Kader El-TanamlyОценок пока нет
- Ooa 00229Документ4 страницыOoa 00229fatma522Оценок пока нет
- Risk Factors For Incident Retinopathy in A Diabetic and Nondiabetic Population - The Hoorn StudyДокумент8 страницRisk Factors For Incident Retinopathy in A Diabetic and Nondiabetic Population - The Hoorn StudyspaceОценок пока нет
- ArticleДокумент7 страницArticleQuentin LISANОценок пока нет
- Jurnal HTДокумент8 страницJurnal HTseruniallisaaslimОценок пока нет
- Hypertension and Hemodialysis: Pathophysiology and Outcomes in Adult and Pediatric PopulationsДокумент12 страницHypertension and Hemodialysis: Pathophysiology and Outcomes in Adult and Pediatric PopulationsinaОценок пока нет
- Righi (2016)Документ6 страницRighi (2016)PelagyalОценок пока нет
- 49 FullДокумент7 страниц49 FullPetru GlavanОценок пока нет
- PPHNДокумент6 страницPPHNHarish SudarsananОценок пока нет
- Controlled Level and Variability of Systolic Blood Pressure On TheДокумент7 страницControlled Level and Variability of Systolic Blood Pressure On TheJeanette LuevanosОценок пока нет
- Seminar: Epidemiology and Risk FactorsДокумент17 страницSeminar: Epidemiology and Risk FactorsNelly ElizabethОценок пока нет
- Effects of Different Antihypertensive Drug Combinations On Blood Pressure and Arterial StiffnessДокумент6 страницEffects of Different Antihypertensive Drug Combinations On Blood Pressure and Arterial StiffnessbimaОценок пока нет
- Hipertensión SitémicaДокумент12 страницHipertensión SitémicaIván Alejandro Trejo ValdiviezoОценок пока нет
- Modern Management of Obstructive Sleep ApneaОт EverandModern Management of Obstructive Sleep ApneaSalam O. SalmanОценок пока нет
- Nutrition in Pregnancy Royal College of Obstetricians and GynaecologistДокумент7 страницNutrition in Pregnancy Royal College of Obstetricians and GynaecologistmeikisirmanОценок пока нет
- AKP 1.2.B.2 Formulir Deteksi Dini Covid 19Документ1 страницаAKP 1.2.B.2 Formulir Deteksi Dini Covid 19meikisirmanОценок пока нет
- Jurnal Reading Retinopati Diabetik Stase MataДокумент16 страницJurnal Reading Retinopati Diabetik Stase MatameikisirmanОценок пока нет
- Refrat: Osteoarthrisis Desti Omega, S.Ked Meiki Permatasari, S.KedДокумент10 страницRefrat: Osteoarthrisis Desti Omega, S.Ked Meiki Permatasari, S.KedmeikisirmanОценок пока нет
- I Am A Filipino by Carlos RomuloДокумент7 страницI Am A Filipino by Carlos RomuloKimberly NgОценок пока нет
- AIKINS v. KOMMENDAДокумент6 страницAIKINS v. KOMMENDAMENSAH PAULОценок пока нет
- Blood TestsДокумент3 страницыBlood TestsMarycharinelle Antolin MolinaОценок пока нет
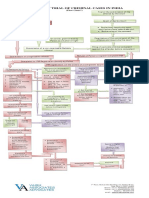
- Process of Trial of Criminal Cases in India (Flow Chart)Документ1 страницаProcess of Trial of Criminal Cases in India (Flow Chart)Arun Hiro100% (1)
- CVT / TCM Calibration Data "Write" Procedure: Applied VehiclesДокумент20 страницCVT / TCM Calibration Data "Write" Procedure: Applied VehiclesАндрей ЛозовойОценок пока нет
- Italian Companies Eastern China - JAN 2014Документ139 страницItalian Companies Eastern China - JAN 2014AndresОценок пока нет
- Coin Operated Short Movie AnalysisДокумент17 страницCoin Operated Short Movie AnalysisA 29 Nathaniela Devany MiramaОценок пока нет
- 6 Cathay vs. VazquezДокумент2 страницы6 Cathay vs. VazquezErwin BernardinoОценок пока нет
- Theory of Design 2Документ98 страницTheory of Design 2Thirumeni MadavanОценок пока нет
- JBL Tune 115TWS HeadphoneДокумент2 страницыJBL Tune 115TWS HeadphoneTimiОценок пока нет
- Assignment # (02) : Abasyn University Peshawar Department of Computer ScienceДокумент4 страницыAssignment # (02) : Abasyn University Peshawar Department of Computer ScienceAndroid 360Оценок пока нет
- Comics Trip MasterpiecesДокумент16 страницComics Trip MasterpiecesDaniel Constantine100% (2)
- Medical and Health Care DocumentДокумент6 страницMedical and Health Care Document786waqar786Оценок пока нет
- Untitled PresentationДокумент23 страницыUntitled Presentationapi-543394268Оценок пока нет
- MEM Companion Volume Implementation Guide - Release 1.1Документ23 страницыMEM Companion Volume Implementation Guide - Release 1.1Stanley AlexОценок пока нет
- 659.69 BM67 2018-02-06 02 Im Beu-UsaДокумент88 страниц659.69 BM67 2018-02-06 02 Im Beu-UsaIrakli JibladzeОценок пока нет
- Agricultural LocationДокумент26 страницAgricultural LocationPrince MpofuОценок пока нет
- Shanu Return Ticket To Sobani HostelДокумент1 страницаShanu Return Ticket To Sobani HostelTamseel ShahajahanОценок пока нет
- SMEC01 CBRS Guide For NBC Reports - v1.1Документ53 страницыSMEC01 CBRS Guide For NBC Reports - v1.1phal sovannarithОценок пока нет
- Form Seven PlacementsДокумент26 страницForm Seven PlacementsRL Iroga100% (4)
- Welcome To UnixДокумент14 страницWelcome To UnixSrinivas KankanampatiОценок пока нет
- PolygonsДокумент23 страницыPolygonsPietrelle Liana PuruggananОценок пока нет
- Huawei Videoconferencing MCU VP9600 Series Data SheetДокумент2 страницыHuawei Videoconferencing MCU VP9600 Series Data SheetIsaac PiresОценок пока нет
- Argumentative Essay-2Документ4 страницыArgumentative Essay-2api-385385980Оценок пока нет
- Room Air Conditioner: Service ManualДокумент68 страницRoom Air Conditioner: Service Manualervin0% (1)
- MVP Teacher 12Документ6 страницMVP Teacher 12Ivan ChuОценок пока нет
- Jaringan Noordin M. TopДокумент38 страницJaringan Noordin M. TopgiantoОценок пока нет
- Pineapple Working PaperДокумент57 страницPineapple Working PaperAnonymous EAineTiz100% (7)
- Prgm-Sminr Faculties Identified Through FIP NIRCДокумент9 страницPrgm-Sminr Faculties Identified Through FIP NIRCDonor CrewОценок пока нет