Вам также может понравиться
- Intervertebral Disc TissuesДокумент30 страницIntervertebral Disc TissuesarlinieОценок пока нет
- CH Turner - Bone StrengthДокумент18 страницCH Turner - Bone Strengthsharathr22Оценок пока нет
- Shoulder: Mohamud DayaДокумент32 страницыShoulder: Mohamud Dayamontserrat santiago sanchezОценок пока нет
- BiomechanicsДокумент41 страницаBiomechanicsRohith Jayasimha Rao100% (1)
- 1 s2.0 S8756328207006205 MainДокумент12 страниц1 s2.0 S8756328207006205 Mainhakan sonsuzlukluОценок пока нет
- Age-Related Changes in The Plasticity and ToughnessДокумент7 страницAge-Related Changes in The Plasticity and ToughnessleonidОценок пока нет
- See Man 2003Документ7 страницSee Man 2003ansoktaОценок пока нет
- Pelvic TraumaДокумент11 страницPelvic TraumaБека ЭзугбаяОценок пока нет
- Pelvic TraumaДокумент11 страницPelvic TraumaEdwardRazvanОценок пока нет
- TraumaДокумент15 страницTraumaPrincess MiraОценок пока нет
- Finite Element Investigation of The Loadin Grate Effect On The Spinal Load-Sharing Changes Under Impact ConditionsДокумент11 страницFinite Element Investigation of The Loadin Grate Effect On The Spinal Load-Sharing Changes Under Impact ConditionsNico FranckОценок пока нет
- Bryce2008 PDFДокумент14 страницBryce2008 PDFsoylahijadeunvampiroОценок пока нет
- AnatomyДокумент9 страницAnatomyannora daffaОценок пока нет
- Current Perspectives On Elbow Dislocation and InstabilityДокумент15 страницCurrent Perspectives On Elbow Dislocation and InstabilityAnonymous L9D1I7DZОценок пока нет
- Crack Effect On Human Femur Bone Under Axial LoadДокумент8 страницCrack Effect On Human Femur Bone Under Axial Loadالراصد طبيОценок пока нет
- Obs-13 240122 184549Документ51 страницаObs-13 240122 184549Edison MesacheОценок пока нет
- Temporomandibular Joint Soft Tissue Pathology-Disc AbnormalitiesДокумент13 страницTemporomandibular Joint Soft Tissue Pathology-Disc AbnormalitiesHassan JaleelОценок пока нет
- MRI of The Posterolateral Corner Injury: A Concise ReviewДокумент6 страницMRI of The Posterolateral Corner Injury: A Concise ReviewIntanОценок пока нет
- Lesiones en LCMДокумент21 страницаLesiones en LCMDiego Quidequeo ReffersОценок пока нет
- 130 January-February 2018Документ2 страницы130 January-February 2018George MogaОценок пока нет
- Amis 2012Документ8 страницAmis 2012abdo houamerОценок пока нет
- Ebacher2007 Dynamic Cimp TractДокумент11 страницEbacher2007 Dynamic Cimp Tractimen mehriОценок пока нет
- Medicon 04Документ5 страницMedicon 04Elisabetta ZanettiОценок пока нет
- Fractura Por Carga AxialДокумент2 страницыFractura Por Carga AxialMBОценок пока нет
- Actures & DislocationsДокумент16 страницActures & Dislocationssabina_grapiniОценок пока нет
- Correlation Compression The Proximal External Degeneration: OF Gross OFДокумент10 страницCorrelation Compression The Proximal External Degeneration: OF Gross OFtrutiОценок пока нет
- Jeffery 2010Документ20 страницJeffery 2010Bianca SantanaОценок пока нет
- Nihms 743965Документ25 страницNihms 743965registrepremsaОценок пока нет
- Comparative Static Analysis For Effect of Linear, Triangular Structural Core Ply MaterialsДокумент7 страницComparative Static Analysis For Effect of Linear, Triangular Structural Core Ply MaterialsGANESH KUMARОценок пока нет
- Muscle Contraction: 126 January-February 2018Документ2 страницыMuscle Contraction: 126 January-February 2018George MogaОценок пока нет
- The Biomechanics of The PC-Fix Internal Fixator: Summary)Документ6 страницThe Biomechanics of The PC-Fix Internal Fixator: Summary)VadymОценок пока нет
- Fractures Part I: Physiology of The Bone 1. Biochemistry of BoneДокумент29 страницFractures Part I: Physiology of The Bone 1. Biochemistry of BoneDaisyyhyОценок пока нет
- Gender-Specific Reproductive Tissue in Ratites and Tyrannosaurus RexДокумент5 страницGender-Specific Reproductive Tissue in Ratites and Tyrannosaurus RexnomadОценок пока нет
- Bone PDFДокумент27 страницBone PDFAndreea HateganОценок пока нет
- Functional Anatomy of The SpineДокумент14 страницFunctional Anatomy of The SpinebandiiitzОценок пока нет
- Orthopedic Hardware and ComplicationsДокумент15 страницOrthopedic Hardware and ComplicationsItstineeОценок пока нет
- Norm Anatomy Elbow 2011Документ11 страницNorm Anatomy Elbow 2011Екатерина БербецОценок пока нет
- Clinical BiomechanicsДокумент4 страницыClinical Biomechanicssulimandaraghmeh1Оценок пока нет
- Hombro Inlges PDFДокумент6 страницHombro Inlges PDFOscar Segun DoОценок пока нет
- Biomechanics of The AnkleДокумент9 страницBiomechanics of The AnkleSanh NguyễnОценок пока нет
- 3 Muscle and ForcesДокумент48 страниц3 Muscle and ForcesNicolas EncisoОценок пока нет
- Depth of Cup and Acetabular OffsetДокумент3 страницыDepth of Cup and Acetabular OffsethaminatrafОценок пока нет
- Mid Shaft Femur FXДокумент10 страницMid Shaft Femur FXDoctor's BettaОценок пока нет
- Chapter 59 - Fracturi Maleola - MTOSДокумент76 страницChapter 59 - Fracturi Maleola - MTOSFlorin MacarieОценок пока нет
- 2nd LabДокумент7 страниц2nd Labahmad mobarkiОценок пока нет
- Femoral Shaft Fractures in AdultsДокумент12 страницFemoral Shaft Fractures in AdultsDiego BellingОценок пока нет
- Wehrli - 2013 - Magnetic ResДокумент14 страницWehrli - 2013 - Magnetic ResHuo ZimuОценок пока нет
- Gender-Specific Reproductive Tissue in Ratites and Tyrannosaurus RexДокумент6 страницGender-Specific Reproductive Tissue in Ratites and Tyrannosaurus RexVitaliy T.Оценок пока нет
- Claes 1999Документ12 страницClaes 1999Bastion ReinhartОценок пока нет
- Soft Tissue Balance KneeДокумент10 страницSoft Tissue Balance KneeNitin BansalОценок пока нет
- The Optimum Temporo-Mandibular Joint Condyle Position in Clinical Practice.Документ26 страницThe Optimum Temporo-Mandibular Joint Condyle Position in Clinical Practice.Jose L LlanosОценок пока нет
- Anatomy of The Anterior Cruciate LigamentДокумент10 страницAnatomy of The Anterior Cruciate LigamentMohamed Faouzi DjidiОценок пока нет
- Bone Mechanical Properties in Healthy and Diseased StatesДокумент31 страницаBone Mechanical Properties in Healthy and Diseased StatesThauane MaiaОценок пока нет
- Remodeling of Femoral StemДокумент24 страницыRemodeling of Femoral StemdabeeraliОценок пока нет
- How To Build Your DragonДокумент17 страницHow To Build Your DragonAllastair Von ToussaintОценок пока нет
- Anatomy and Biomechanics of The Cruciate Ligaments and Their Surgical ImplicationsДокумент12 страницAnatomy and Biomechanics of The Cruciate Ligaments and Their Surgical ImplicationsMd Ahsanuzzaman PinkuОценок пока нет
- Netter Anatomy Section 6-LOWER LIMBДокумент100 страницNetter Anatomy Section 6-LOWER LIMBRickky MD100% (1)
- Jexbio 27 3 264Документ28 страницJexbio 27 3 264Nikhil JohnОценок пока нет
- The Anatomy of the Horse's Foot and Hoof - A Collection of Historical Articles on the Physiology and Function of the Foot and HoofОт EverandThe Anatomy of the Horse's Foot and Hoof - A Collection of Historical Articles on the Physiology and Function of the Foot and HoofОценок пока нет
- Comminuted Lumbar Vertebral Fracture With Spinal Cord Compromise in An Adolescent Female After A Minor FallДокумент5 страницComminuted Lumbar Vertebral Fracture With Spinal Cord Compromise in An Adolescent Female After A Minor FallBella LimОценок пока нет
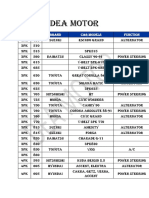
- Dea MotorДокумент10 страницDea MotorBella LimОценок пока нет
- Chest Physical Therapy (CPT: Postural DrainageДокумент6 страницChest Physical Therapy (CPT: Postural DrainageBella LimОценок пока нет
- TOEFL Structure and Written Expression by NargisДокумент19 страницTOEFL Structure and Written Expression by NargisBella LimОценок пока нет
- CPM PPT 2Документ17 страницCPM PPT 2Bella LimОценок пока нет
- 0708 Conduction Convection RadiationДокумент23 страницы0708 Conduction Convection RadiationBella LimОценок пока нет
- Natural ColorДокумент14 страницNatural ColorleeОценок пока нет
- Module 3 HW5Документ14 страницModule 3 HW5hgfhfghfghgОценок пока нет
- 0000 Pi SPC 004Документ18 страниц0000 Pi SPC 004zsmithОценок пока нет
- Prototype To Help The Improvement of E-Toll PaymentДокумент14 страницPrototype To Help The Improvement of E-Toll Paymentfarhan satriyaОценок пока нет
- Worzakowska2016 Article ThermalBehaviorDecompositionMeДокумент10 страницWorzakowska2016 Article ThermalBehaviorDecompositionMeJavier Andres Munoz ChavesОценок пока нет
- Flender Manual GeneralДокумент42 страницыFlender Manual GeneralYenny LaraОценок пока нет
- Matlab For SHRT Circuit AnalysisДокумент6 страницMatlab For SHRT Circuit AnalysisM B Hemanth KumarОценок пока нет
- Potential Difference WorksheetДокумент2 страницыPotential Difference WorksheetDigCity DiggОценок пока нет
- Energy Guide Midea - Mrc07m6aww Mrc07m6ewwДокумент1 страницаEnergy Guide Midea - Mrc07m6aww Mrc07m6ewwharry HendersonОценок пока нет
- Pengaruh Kecepatan Pemotongan Dan Ketebalan Bahan Terhadap Kekerasan Dan Kekasaran Permukaan Baja Aisi 1045 Menggunakan CNC Plasma Arc CuttingДокумент6 страницPengaruh Kecepatan Pemotongan Dan Ketebalan Bahan Terhadap Kekerasan Dan Kekasaran Permukaan Baja Aisi 1045 Menggunakan CNC Plasma Arc CuttingRamjay BudiartoОценок пока нет
- Us2656248 PDFДокумент4 страницыUs2656248 PDFchuckannabelleОценок пока нет
- 3 IdiotsДокумент6 страниц3 IdiotsvonashОценок пока нет
- First Push 2024 Grade 12 Marking Guide March 2024Документ12 страницFirst Push 2024 Grade 12 Marking Guide March 2024lemonlululu1Оценок пока нет
- Sri Chaitanya Physics Integer Type Question BANKkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkДокумент74 страницыSri Chaitanya Physics Integer Type Question BANKkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkkSai GokulОценок пока нет
- Surface PlateДокумент3 страницыSurface PlateSaket OraonОценок пока нет
- Power System Engineering MaterialДокумент6 страницPower System Engineering MaterialAshok SainiОценок пока нет
- Data Compression TechniquesДокумент20 страницData Compression TechniquesAbhishek kumar singh100% (2)
- DM Water Tank SpecificationДокумент9 страницDM Water Tank SpecificationManish PatelОценок пока нет
- St501-Ln1kv 04fs EnglishДокумент12 страницSt501-Ln1kv 04fs Englishsanthoshs241s0% (1)
- Energy, Energy Transfer, and General Energy AnalysisДокумент23 страницыEnergy, Energy Transfer, and General Energy AnalysisBen RileyОценок пока нет
- Foaming in The Cooling Tower - FlatДокумент1 страницаFoaming in The Cooling Tower - FlatJavier GonzalezОценок пока нет
- Sheldon S File 3Документ7 страницSheldon S File 3NATHANIEL YACASОценок пока нет
- Use Pipet To Add Exactly The Same of The 0.1% Indicator Solution 0.50mL Is A Suitable VolumeДокумент4 страницыUse Pipet To Add Exactly The Same of The 0.1% Indicator Solution 0.50mL Is A Suitable Volume林鴻鈞Оценок пока нет
- 40C Lab 3 Capacitors8Документ8 страниц40C Lab 3 Capacitors8Desiree Mae IbonОценок пока нет
- ANSI Relaying Current Transformer BurdenДокумент1 страницаANSI Relaying Current Transformer BurdenbhaskarinvuОценок пока нет
- Hooke's Law (4Документ30 страницHooke's Law (4Clark Harold Balido50% (2)
- Xilinx Spartan3 Device ReliabilityДокумент118 страницXilinx Spartan3 Device ReliabilityRaffi SkОценок пока нет
- Industrial HygieneДокумент29 страницIndustrial Hygieneghoshna jyotiОценок пока нет
- Cross Taping - A Practical Guide 12Документ2 страницыCross Taping - A Practical Guide 12jfjjfjfjjfjfОценок пока нет
- Water Stagnant of Solar ModulesДокумент6 страницWater Stagnant of Solar ModulesNITIN MISHRAОценок пока нет