Articles
Comparative effectiveness and cost-effectiveness of
treat-to-target versus benefit-based tailored treatment of
type 2 diabetes in low-income and middle-income countries:
a modelling analysis
Sanjay Basu, Vishnu Shankar, John S Yudkin
Summary
Lancet Diabetes Endocrinol 2016; Background Optimal prescription of blood pressure, lipid, and glycaemic control treatments for adults with type 2
4: 922–32 diabetes remains unclear. We aimed to compare the effectiveness and cost-effectiveness of two treatment approaches
Published Online for diabetes management in five low-income and middle-income countries.
October 4, 2016
http://dx.doi.org/10.1016/
S2213-8587(16)30270-4 Methods We developed a microsimulation model to compare a treat-to-target (TTT) strategy, aiming to achieve target
See Comment page 879
levels of biomarkers (blood pressure <130/80 mm Hg, LDL <2·59 mmol/L, and HbA1c <7% [ie, 53∧0 mmol/mol]),
Department of Medicine,
with a benefit-based tailored treatment (BTT) strategy, aiming to lower estimated risk for complications (to a 10 year
Stanford University, Palo Alto, cardiovascular risk <10% and lifetime microvascular risk <5%) on the basis of age, sex, and biomarker values. Data
CA, USA (S Basu PhD, were obtained from cohorts in China, Ghana, India, Mexico, and South Africa to span a spectrum of risk profiles.
V Shankar); Center for Primary
Care, Harvard Medical School,
Boston, MA, USA (S Basu); and
Findings The TTT strategy recommended treatment to a larger number of people—who were generally at lower risk
Division of Medicine, of diabetes complications—than the BTT. The BTT strategy recommended treatment to fewer people at higher risk.
University College London, Compared with the TTT strategy, the BTT strategy would be expected to avert 24·4–30·5% more complications and
London, UK (J S Yudkin MD) be more cost-effective from a societal perspective (saving US$4·0–300·0 per disability-adjusted life-year averted in
Correspondence to: the countries simulated). Alternative treatment thresholds, matched by total cost or population size treated, did not
Dr Sanjay Basu, Stanford
University, 1070 Arastradero
change the comparative superiority of the BTT strategy, nor did titrating treatment using fasting plasma glucose (for
Road, Office 282, Palo Alto, areas without HbA1c testing). However, if insulin were unavailable, the BTT strategy would no longer be superior for
CA 94304, USA preventing microvascular events and was superior only for preventing cardiovascular events.
basus@stanford.edu
Interpretation A BTT strategy is more effective and cost-effective than a TTT strategy in low-income and middle-
income countries for prevention of both cardiovascular and microvascular complications of type 2 diabetes. However,
the superiority of the BTT strategy for averting microvascular complications is contingent on insulin availability.
Funding Rosenkranz Prize for Healthcare Research in Developing Countries and US National Institutes of Health
(U54 MD010724, DP2 MD010478).
Introduction basis of composite estimates of cardiovascular risk,
Treatment of type 2 diabetes is required for an increasing which incorporate numerous inter-related risk factors
number of people worldwide as the prevalence of (eg, age, sex, tobacco smoking, blood pressure, and lipid
diabetes continues to rise.1 Such treatment in low-income profile) rather than LDL concentrations alone.7,8 A similar
and middle-income countries, in particular, requires shift for blood pressure treatment decisions has been
careful consideration of how to maximise the benefits proposed by Rod Hayward and colleagues since 2013,9,10
for the largest number of patients within highly in view of accumulating evidence from randomised trials
constrained budgets. that composite estimates of cardiovascular risk are a
Treatment of type 2 diabetes requires management of better predictor of treatment benefits than systolic or
three principal, coexisting risk factors for morbidity and diastolic blood pressure alone.11–13 Less well studied is the
mortality: high blood pressure, dyslipidaemia, and poor idea of extending a BTT strategy to glycaemic control,
glycaemic control.2–4 Management of these three risk since some patients have a greater microvascular risk
factors has traditionally been guided by a treat-to-target reduction than others from the same decline in HbA1c
(TTT) strategy focused on achieving specific levels of concentrations.14,15 Whether TTT or BTT is a better
blood pressure, LDL cholesterol, and HbA1c.5 In 2014, treatment approach for averting both cardiovascular and
reflecting the concern that LDL concentrations are an microvascular complications in people with type 2
imperfect marker for patients who will benefit from diabetes remains unclear.
statin treatment, US practice guidelines shifted towards Treatment benefits for people with type 2 diabetes
a benefit-based tailored treatment (BTT) strategy6— depend on interactions between glycaemic control and
directing clinicians to prescribe statin treatment on the management of high blood pressure, dyslipidaemia, and
922 www.thelancet.com/diabetes-endocrinology Vol 4 November 2016
Articles
Research in context
Evidence before this study low-income and middle-income countries, a BTT approach to
Two authors (SB and VS) independently searched PubMed and blood pressure treatment was shown to be more effective and
Google Scholar for English-language articles with the keywords cost-effective than a TTT approach for prevention of
“treatment targets”, “personalized treatment”, “risk-based cardiovascular diseases.
therapy”, or “benefit-based tailored therapy”, along with the
Added value of this study
keyword “diabetes” from Jan 1, 1980, to July 31, 2016. Based
By contrast with previous studies, we directly compared the TTT
on consensus discussion, we reviewed four relevant papers on
and BTT strategies in people with type 2 diabetes in five
treat-to-target (TTT) and benefit-based tailored treatment
low-income and middle-income countries. Our findings reveal
(BTT) strategies for diabetes management. Findings from two
that a BTT strategy for blood pressure, lipid, and glycaemic
studies involving simulation models of the US population
control would be more effective and cost-effective than a TTT
suggested that, for lipid and blood pressure treatment, a BTT
strategy for prevention of both cardiovascular and
strategy would be more effective and cost-effective than a TTT
microvascular complications of type 2 diabetes. However, the
strategy for patients without diabetes. In another study, a
superiority of the BTT strategy for averting microvascular
simulation model of US populations with type 2 diabetes
complications would necessitate insulin availability.
showed that, for most patients older than 50 years with HbA1c
less than 9% and receiving metformin, additional glycaemic Implications of all the available evidence
treatment usually offers modest benefits, supporting Our findings imply that global guidelines for type 2 diabetes
treatment based on a comprehensive consideration of risk therapy should consider a BTT approach rather than a TTT
rather than a universal target for HbA1c. Finally, in another approach for cardiovascular disease prevention, and also for
study using a simulation of people without diabetes in microvascular disease prevention where insulin is available.
other comorbidities.2–4,16 Hence, whether and under what Bank criteria,18 spanning a global spectrum of risk
circumstances a TTT or BTT approach would provide profiles: China, Ghana, India, Mexico, and South Africa.
more benefits to people with type 2 diabetes remains We included parameters for UN population projections
unclear. The treatment strategies followed by clinicians by age, sex, and urban versus rural residence by country;19
will have profound implications for who receives age distribution and secular trends in prevalence of type
treatment, how well the treatment averts diabetes 2 diabetes from the International Diabetes Federation;20
complications and related disability, and overall and risk factors for cardiovascular and microvascular
programme cost and cost-effectiveness—all of which are complications from cohorts including people with type 2
key considerations for government ministers evaluating diabetes in each country (particularly the WHO study on
whether and how to pay for treatment.17 global ageing and adult health in 2007–10),21
In this study, we sought to compare both the effectiveness supplemented by a PubMed search to ensure that a
and cost-effectiveness of TTT and BTT approaches for broad range of possible values were incorporated
diabetes management in five low-income and (appendix pp 9–12). The estimated prevalence of type 2 See Online for appendix
middle-income countries using a microsimulation model. diabetes was 9·3% in China, 2·2% in Ghana, 8·8% in
India, 15·0% in Mexico, and 7·2% in South Africa,
Methods compared with 14·3% in the USA and 12·4% in the UK
Model structure in populations of the same age group.20,22,23 The WHO
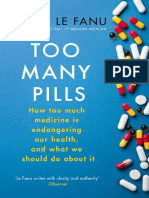
We constructed a microsimulation model (figure) to study on global ageing and adult health21 included
simulate adults aged 20–79 years and their risks of five 3993 individuals in China, 3938 in Ghana, 9994 in India,
major diabetes complications: the cardiovascular 38 746 in Mexico, and 2352 in South Africa. Within each
complications of myocardial infarction and stroke, and the country, we simulated a representative age-adjusted
microvascular complications of end-stage renal disease, population of 100 000 people with type 2 diabetes.24 We
blindness, and diabetic ulcer. We chose a microsimulation then used equations from the internationally validated
approach over a traditional Markov cohort approach UK Prospective Diabetes Study outcomes model
because microsimulation captures the correlations version 2 (UKPDS OM2)25,26 to estimate ethnicity-specific
between individual demographic characteristics, risk risk of each complication over the full simulated lifetime
factors, and complication rates. Therefore, we could of each individual given a simulated individual’s risk
account for important variations in risk within each factors, including systolic blood pressure, lipid profile,
country’s population (which was necessary for simulating HbA1c concentration, tobacco smoking, BMI, and
the BTT approach), rather than only simulating the glomerular filtration rate. Mortality by age, sex, and
population average risk of complications. country was incorporated from WHO estimates
Our model included high-quality data from five (appendix p 13). Complete details on model programming
countries classified as low or middle income by World are given in the appendix.
www.thelancet.com/diabetes-endocrinology Vol 4 November 2016 923
Articles
Comparative effectiveness analysis treatment with metformin, a sulfonylurea and, if needed,
Under the TTT strategy, we simulated the following insulin replacing the sulfonylurea to achieve a lifetime
recommended treatment for people with type 2 diabetes: combined risk of the major microvascular complications
first, a statin with dose titration to achieve a LDL of less than 5% (as long as fasting plasma glucose
concentration of less than 2·59 mmol/L (ie, 100 mg/dL);27 remained at least 3·33 mmol/L [ie, 60 mg/dL] for safety),
second, blood pressure-lowering agents to achieve a with additional blood pressure-lowering agents and a
blood pressure of less than 130/80 mm Hg;28 third, statin prescribed to achieve the microvascular goal if it was
metformin, a sulfonylurea and, if needed, insulin not achieved through glycaemic control alone (with blood
replacing the sulfonylurea to achieve a HbA1c pressure maintained at 110/55 mm Hg or above; figure).
concentration of less than 7% (ie, 53∧0 mmol/mol; The sequence of treatment in the BTT strategy was chosen
figure).5 Testing of alternative targets was done as part of to maximise relative risk reduction for mortality in people
the sensitivity analyses (see below). We followed WHO with type 2 diabetes, hence the strategy conferring the
guidelines when adopting medication choices (including greatest relative risk reduction was ordered first and the
isophane insulin as basal insulin, with regular insulin smallest relative risk reduction last (appendix pp 2–4).
for prandial coverage as needed), and simulated dose Single-dose statin therapy, ordered first in the BTT
effects on biomarkers and the risk of each complication protocol, was chosen because of previous work justifying
based on meta-analyses of randomised trials (appendix this empirical dosing approach and because of limited
pp 2–4).28–33 The TTT strategy attempts to achieve each of availability of alternative statins and statin doses in low-
the targets independently, such that an individual with income and middle-income countries.34,36,37
normal blood pressure would not require blood pressure-
lowering treatment but might require statin and Cost-effectiveness analysis
glycaemic control treatment. According to cost-effectiveness analysis guidelines,38,39 we
Under the BTT strategy, we envisioned that simulated the complete life-course of all people alive or
cardiovascular and microvascular risk could be assessed by born who have or develop type 2 diabetes during the next
risk tables (see appendix p 29 for an example of a 10 years (2016–25).24,40 We integrated treatment costs from
microvascular risk table) based on the UKPDS OM2 a societal perspective (regardless of payer) and expressed
equations,25 similar to WHO guideline charts displaying cost-effectiveness ratios as discounted costs over
cardiovascular risk by patient demographics and biomarker discounted disability-adjusted life-years (DALYs) at a
values.28 We simulated the following recommended 3% annual discount rate. We first calculated mean cost-
treatments: first, statin treatment with simvastatin 40 mg effectiveness ratios for both TTT and BTT, with no
daily if an individual’s 10 year baseline cardiovascular risk treatment as the comparator scenario, to correspond to
(ie, combined risk of myocardial infarction and stroke) was WHO CHOICE guidelines and in view of the lack of data
at least 10%;34 second, subsequent addition of blood on present treatment access levels. We also calculated
pressure-lowering agents to achieve a 10 year combined incremental cost-effectiveness ratios if TTT was switched
risk of myocardial infarction and stroke of less than 10% to BTT at full availability and coverage. We calculated
(provided that blood pressure remained at least at DALYs using disability weight values estimated by the
110/55 mm Hg for safety);35 and third, glycaemic control Global Burden of Disease Study,41 drug costs for therapy
in all countries based on per-unit buyer cost estimates
from the International Drug Price Indicator Guide,42 and
assay and service cost data based on published field
Decide therapy based Treat to blood pressure surveys (appendix p 14). We expressed all costs in 2016
Treat-to-target on biomarkers (blood <130/80 mm Hg,
strategy pressure, LDL, and HbA1c) LDL <2·59 mmol/L, US dollars. The Consolidated Health Economic
and HbA1c <7% Evaluation Reporting Standards (CHEERS) checklist is
shown in the appendix p 31–33.
Estimate probability of: Sensitivity analyses
Simulate risk factors • Myocardial infarction We did six sensitivity analyses. First, we varied the BTT
in population with • Stroke
type 2 diabetes • Blindness glycaemic treatment threshold from a baseline of
• End-stage renal disease 5% lifetime microvascular risk to thresholds of 3% and
• Ulcer
7% risk. Second, we changed the TTT glycaemic
biomarker from HbA1c to fasting plasma glucose (target
<7 mmol/L, according to WHO guidance28) to reflect the
Decide therapy based Treat to 10 year
Benefit-based tailored on cardiovascular and cardiovascular risk <10% unavailability of HbA1c assay in some areas. Third, we set
treatment strategy microvascular risk estimates and lifetime the BTT treatment thresholds to produce the same total
microvascular risk <5%
number of people treated as the TTT strategy within
each country (where the number treated includes any
Figure: Model diagram form of treatment—any blood pressure-lowering agent,
924 www.thelancet.com/diabetes-endocrinology Vol 4 November 2016
Articles
China Ghana India Mexico South Africa
(prevalence 9·3%) (prevalence 2·2%) (prevalence 8·8%) (prevalence 15·0%) (prevalence 7·2%)
Age at diagnosis, years 57·5 (53·6 to 61·4) 54·0 (50·1 to 57·9) 56·0 (52·1 to 60·0) 52·4 (48·5 to 56·3) 54·0 (50·1 to 57·9)
Systolic blood pressure, mm Hg 141·1 (120·1 to 165·0) 144·4 (119·9 to 173·8) 143·7 (119·2 to 173·3) 143·0 (118·7 to 173·3) 143·1 (118·6 to 172·5)
LDL, mmol/L 2·9 (1·8 to 4·2) 3·0 (1·9 to 4·3) 3·1 (1·9 to 4·5) 3·0 (1·9 to 4·3) 3·0 (1·9 to 4·3)
HbA1c 8·2% (6·2 to 12·2) 8·7% (6·6 to 13·0) 8·4% (6·3 to 12·5) 9·0% (6·8 to 13·4) 8·7% (6·6 to 13·0)
History of cardiovascular diseases 21·4% (10·7 to 42·8) 16·4% (8·2 to 32·8) 17·1% (8·6 to 34·2) 10·8% (5·4 to 21·6) 22·2% (11·1 to 44·4)
10 year cardiovascular disease risk 25·4% (4·4 to 77·6) 24·4% (4·4 to 74·0) 26·3% (4·7 to 79·2) 25·3% (4·3 to 77·0) 25·5% (4·5 to 77·2)
Lifetime microvascular risk 17·2% (4·1 to 58·7) 17·9% (4·3 to 60·2) 19·9% (4·5 to 67·9) 16·3% (4·0 to 53·7) 15·5% (4·0 to 50·0)
Data are mean (95% CI).
Table 1: Pre-treatment patient characteristics
statin, or glycaemic control agent). Fourth, we simulated Compared with the TTT strategy, the BTT strategy would
the scenario in which insulin was unavailable (ie, only be expected to avert 24·4–30·5% more complications and
metformin and sulfonylurea were available). Fifth, we therefore had a significantly lower number needed to treat
simulated outcomes if the BTT guidelines had a 10% within each country (ranging from 22·9 to 25·0 for TTT vs
lower adherence from practitioners than the TTT 15·4 to 17·1 for BTT for cardiovascular events, and 64·0 to
scenario to reflect practitioner resistance to change from 81·1 vs 57·1 to 70·3 for microvascular events; table 2).
the conventional TTT approach. Finally, we simulated The BTT strategy would be expected to avert significantly
outcomes of combining the BTT approach for preventing more complications for all outcomes measured (40–53%
cardiovascular complications with the TTT approach for more myocardial infarctions, 38–53% more strokes,
preventing microvascular complications. 25–33% more blindness cases, and 12–15% more end-
In all scenarios, we performed discrete sensitivity stage renal diseases), with the exception of diabetic ulcers,
analyses by repeating each country-specific simulation for which the difference between the two strategies was
10 000 times, repeatedly sampling with replacement from not significant (table 2). The proportions of complications
normal distributions constructed around all input averted by the TTT strategy (calculated by comparing TTT
parameter estimates to estimate 95% CIs. The analysis with the no-treatment scenario) averaged 14% for
included uncertainty in the risk equation coefficients to myocardial infarctions, 17% for strokes, 6% for blindness,
account for the imprecision and potential errors involved 6% for renal failure, and 19% for ulcers; the proportion
in risk estimation, and subsequent consequences for averted by the BTT strategy averaged 21% for myocardial
patient outcomes. We performed simulations in R, infarctions, 26% for strokes, 9% for blindness, 7% for
version 3.2. renal failure, and 19% for ulcers.
Compared with the TTT strategy, the BTT strategy had
Role of the funding source equivalent cost but significantly greater effectiveness
The funder of the study had no role in study design, data (ie, averted significantly more DALYs) in all countries
collection, data analysis, data interpretation, or writing of studied (table 2). The absolute costs of both strategies
the report. The corresponding author had full access to ranged from $517·6 to $1020·1 per person per year in
all the data in the study and had final responsibility for the studied countries because of variations in
the decision to submit for publication. medication costs (with 11% of total costs from blood
pressure-lowering agents, statins, and glycaemic control
Results agents, including 4% of total costs from insulin) and
Pre-treatment patient characteristics are shown in health-care service costs (with 55% of total costs from
table 1. In all five countries modelled, the TTT strategy microvascular disease management costs such as
would recommend treatment to a larger proportion of dialysis and ulcer treatment, and the remainder from
patients with type 2 diabetes than would the BTT cardiovascular disease management costs post
strategy (table 2). Whereas the TTT strategy would myocardial infarction or stroke across all five countries).
recommend at least one form of treatment (at least one The BTT strategy averted 0·016–0·038 more DALYs per
blood pressure, lipid, or glycaemic control agent) to person per year than did the TTT strategy. Compared
99·1–99·4% of patients, the BTT strategy would with no treatment, the BTT strategy had a mean cost-
recommend treatment to 96·4–98·1% of patients (ie, effectiveness ratio of $7215·9–12 038·8 per DALY
1·2–2·9% fewer people). However, the TTT strategy averted across the studied countries, whereas for the
would recommend fewer medications per person treated TTT strategy the mean cost-effectiveness ratio ranged
(3·0–3·3), meaning that the BTT strategy would more from $10 448·7 to $16 710·4 per DALY averted and was
intensely treat a smaller population of patients higher than that of the BTT strategy in all countries
(3·7–3·8 medications per person treated). modelled. The incremental cost-effectiveness ratio of
www.thelancet.com/diabetes-endocrinology Vol 4 November 2016 925
Articles
shifting from the TTT strategy to the BTT strategy strategy, or vice versa (table 3). Patients who were more
varied from –$4·0 to –$300·0 per incremental DALY likely to have a complication averted by the TTT strategy
averted across the studied countries, indicating cost- than the BTT strategy were substantially younger (by
savings from the BTT strategy (table 2). 6·2 years on average) and more likely to be female
We compared patients prevented from diabetes-related (19·8% more women than men; table 3). Generally, those
complications by the two treatment approaches, in terms averted from a complication by the TTT strategy but not
of their pre-treatment characteristics, to identify whether the BTT strategy were also of lower risk (4·0% lower
any factors substantially differed between the groups, or 10 year cardiovascular risk and 4·4% lower lifetime
whether any particular biomarkers could predict which microvascular risk; table 3).
patient subgroups would benefit more from one strategy To further compare the effectiveness and efficiency of
versus the other. We did not observe any biomarker that medications in the two approaches, we compared risks
could predict which patients would be prevented from a and outcomes in patients treated more intensively
complication by the TTT strategy and not the BTT (ie, with more medications) under the TTT strategy with
China Ghana India Mexico South Africa
TTT BTT TTT BTT TTT BTT TTT BTT TTT BTT
Treatment recommendations
Adults with type 2 99·1% 97·0% 99·4% 97·2% 99·3% 98·1% 99·2% 96·6% 99·3% 96·4%
diabetes on any (99 to 99·1) (97·0 to 97·1) (99·3 to (97·1 to 97·2) (99·2 to 99·4) (98 to 98·1) (99·2 to 99·3) (96·4 to 96·7) (99·2 to 99·3) (96·4 to 96·5)
recommended 99·4)
treatment
Blood pressure- 80·5% 82·5% 86·4% 81·0% 85·4% 84·4% 84·1% 82·3% 84·1% 82·7%
lowering treatment (80·3 to 80·6) (82·2 to 82·7) (86·3 to 86·6) (80·9 to 81·1) (85·2 to 85·5) (84·2 to 84·5) (83·9 to 84·2) (82·2 to 82·5) (83·8 to 84·3) (82·5 to 82·8)
Lipid control treatment 75·2% 82·8% 75·4% 81·2% 75·3% 84·5% 75·3% 82·5% 75·3% 82·9%
(75·1 to 75·5) (82·5 to 83·0) (75·2 to 75·6) (81 to 81·3) (75·1 to 75·6) (84·3 to 84·7) (75·2 to 75·5) (82·4 to 82·7) (75·0 to 75·5) (82·7 to 83·0)
Glycaemic control 80·7% 92·8% 80·7% 93·8% 80·7% 95·1% 80·7% 92·0% 80·8% 91·9%
treatment (80·5 to 80·9) (92·7 to 92·9) (80·6 to 80·9) (93·7 to 94·0) (80·6 to 80·9) (95 to 95·2) (80·5 to 80·9) (91·8 to 92·1) (80·6 to 81·0) (91·7 to 92·0)
Insulin treatment 13·8% 16·9% 13·8% 17·7% 13·8% 19·3% 13·8% 16·1% 13·8% 15·3%
(13·7 to 13·9) (16·7 to 17·1) (13·7 to 14·0) (17·5 to 17·9) (13·7 to 14·0) (19·1 to 19·4) (13·5 to 13·9) (15·9 to 16·3) (13·7 to 14·0) (15·2 to 15·5)
Number of 3·0 3·8 3·3 3·7 3·2 3·8 3·2 3·7 3·2 3·8
medications, per person (3·0 to 3·1) (3·8 to 3·8) (3·3 to 3·3) (3·7 to 3·7) (3·2 to 3·3) (3·8 to 3·8) (3·2 to 3·2) (3·7 to 3·8) (3·2 to 3·2) (3·8 to 3·8)
on recommended
treatment
Complications and deaths prevented from 10 years of treatment
Cardiovascular events, per 100 000 people
Myocardial 2098·4 3218·9 2206·5 3080·9 2290·4 3390·2 2201·1 3232·2 2200·8 3270·7
infarction (2005·4 to (3145·3 to (2133·2 to (3021·6 to (2229·6 to (3334·5 to (2125·5 to (3153·8 to (2111·3 to (3208·1 to
2146·1) 3299·4) 2268·7) 3197·7) 2356·0) 3471·1) 2311·4) 3343·7) 2309·9) 3335·6)
Stroke 1857·3 2841·4 1885·3 2595·1 2054·4 2967·7 1932·0 2784·0 1941·5 2850
(1771·5 to (2813·1 to (1790·5 to (2539·0 to (1986·8 to (2857·3 to (1886·0 to (2731·7 to (1881·5 to (2791·2 to
1914·8) 2882·8) 1966) 2677·6) 2134·1) 3085·0) 1982·2) 2822·7) 1995·6) 2906)
Microvascular events, per 100 000 people
Blindness 229·4 303·5 244·1 305·7 238·2 310·1 225·2 295·9 222·3 295·1
(214·2 to (286·5 to (228·0 to (285·4 to (219·6 to (284·6 to (205·6 to (274·5 to (204·9 to (266·8 to
240·0) 327·1) 264·8) 328·8) 270·0) 329·0) 242·9) 336·8) 243·7) 319·9)
End-stage renal 764·0 881·7 833·5 955·0 973·7 1110·5 705·4 810·3 590·0 687·5
disease (731·1 to (840·0 to (813·3 to (917·6 to (936·2 to (1065·5 to (675·4 to (785·6 to (559·0 to (649·9 to
799·2) 920·7) 862·9) 989·4) 1020·1) 1155·8) 736·4) 871·6) 614·6) 731·5)
Ulcer 265·3 260·4 261·8 245·1 220·6 200·1 306·1 291·3 411·9 389·7
(238·7 to (243·0 to (239·1 to (217·5 to (198·7 to (177·4 to (258·0 to (278·9 to (369·9 to (357·2 to
286·0) 284·4) 295·5) 262·8) 256·0) 218·7) 345·1) 307·9) 442·6) 425·7)
Deaths, per 100 000 1409·8 2051·7 1467·9 1957·7 1596·8 2214·7 1439·3 2008·8 1404·5 2000·1
people (1346·0 to (2010·0 to (1409·6 to (1910·3 to (1545·0 to (2145·5 to (1394·2 to (1963·7 to (1351·1 to (1950·8 to
1454·3) 2098·6) 1522·3) 2025·7) 1657·7) 2291·7) 1493·5) 2069·1) 1457·3) 2051·3)
Number needed to 25·0 16·0 24·3 17·1 22·9 15·4 24·0 16·1 24·0 15·8
treat to prevent one (24·4 to 26·2) (15·7 to 16·3) (23·5 to 25·3) (16·5 to 17·5) (22·1 to 23·5) (15·0 to 15·8) (23·1 to 24·7) (15·7 to 16·4) (23·1 to 24·8) (15·5 to 16·1)
cardiovascular event
Number needed to 64·0 57·1 74·2 64·5 69·3 60·5 80·2 69·1 81·1 70·3
treat to prevent one (60·8 to 67·8) (54·0 to 60·1) (69·8 to 77·6) (61·5 to 68·4) (64·3 to 73·3) (57·6 to 64·2) (74·9 to 87·1) (63·8 to 72) (76·3 to 87·5) (65·4 to 75·7)
microvascular event
(Table 2 continues on next page)
926 www.thelancet.com/diabetes-endocrinology Vol 4 November 2016
Articles
China Ghana India Mexico South Africa
TTT BTT TTT BTT TTT BTT TTT BTT TTT BTT
(Continued from previous page)
Cost and cost-effectiveness
Total costs, per person $891·1 $886·8 $725·4 $724·6 $952·6 $952·5 $1020·1 $1012·4 $517·6 $512·8
per year (876·6 to (871·2 to (717·4 to (717·7 to (946·8 to (946·3 to (1005·3 to (997·8 to (513·3 to (507·6 to
906·7) 901·0) 735·8) 736·0) 959·0) 958·3) 1035·6) 1028·1) 522·7) 517·3)
Total DALYs averted, 0·085 0·123 0·043 0·060 0·063 0·088 0·093 0·127 0·031 0·047
per person per year (0·083 to (0·121 to (0·042 to (0·059 to (0·062 to (0·087 to (0·091 to (0·125 to (0·031 to (0·046 to
0·087) 0·124) 0·045) 0·061) 0·065) 0·089) 0·095) 0·129) 0·032) 0·048)
Cost-effectiveness $10 448·7 $7215·9 $16 710·4 $12 038·8 $15 124·1 $10 769·1 $11 019·0 $7941·9 $16 448·0 $10 928·4
ratio compared with (10 353·1 to (7209·5 to (16 327·0 to (11 978·3 to (14 800·2 to (10 728·3 to (10 897·4 to (7843·1 to (16 168·6 to (10 754·1 to
no treatment, per 10 514·3) 7254·9) 17 094·0) 12 106·3) 15 385·0) 10 840·7) 11 062·4) 7966·0) 16 728·4) 11 017·3)
DALY averted
Incremental cost- ¨ –$113·2 ¨ –$47·1 ¨ –$4·0 ¨ –$226·5 ¨ –$300·0
effectiveness ratio of (–126·5 to (–57·1 to (–4·5 to –3·7) (–256·7 to (–342·9 to
shifting from TTT to –104·9) –42·1) –202·6) –282·4)
BTT, per incremental
DALY averted
Data are mean (95% CI). Costs are in 2016 US dollars. TTT=target-to-treat. BTT=benefit-based tailored treatment. DALYs=disability-adjusted life-years.
Table 2: Effectiveness and cost-effectiveness of TTT and BTT strategies for reducing complications of type 2 diabetes
those treated more intensively under the BTT strategy effects on the relative difference in either effectiveness or
(table 4). Compared with patients treated more cost-effectiveness between the TTT and BTT strategies
intensively by the BTT strategy, those treated more (appendix pp 19–20). The TTT strategy had slightly
intensively by the TTT strategy had a roughly 12% lower improved outcomes on average, likely because of the
initial 10 year cardiovascular disease risk and 3% lower slightly greater glycaemic control implied by a fasting
initial lifetime microvascular risk on average. Under plasma glucose target of 7 mmol/L versus an HbA1c target
this scenario, the relative cost of treatment by the TTT of 7%, but the confidence intervals under this scenario
strategy was 2·5–3·7 times higher per DALY averted marginally increased because of less consistency in how
than that by the BTT strategy, suggesting lower fasting plasma glucose correlated with long-term
efficiency of the TTT strategy per dollar spent in these microvascular outcomes.
subgroups of patients. Similarly, the treatment efficiency Adjustment of the BTT treatment thresholds such that
of TTT was 13·0–18·8% lower when estimated as DALYs the same total population was treated in each country by
averted per 1000 patient-years of medication dispensed, both strategies (appendix pp 21–22) did not appreciably
with 0·2–0·5 fewer DALYs averted per 1000 patient-years change the comparative results, with the TTT strategy
of medication dispensed compared with the BTT still being inferior in effectiveness and cost-effectiveness
strategy (table 4). across all five countries.
Alteration of the threshold for treating microvascular If insulin were unavailable, the total numbers needed
risk under the BTT strategy from the base case of to treat to prevent a microvascular event increased under
5% lifetime risk to 3% or 7% lifetime risk did not both strategies (appendix pp 23–24), and the BTT strategy
significantly change the effectiveness or cost-effectiveness remained more effective than the TTT strategy for
of the BTT strategy relative to the TTT strategy (appendix cardiovascular outcomes but not for microvascular
pp 15–18); the uncertainty range around risk calculations, outcomes. The TTT strategy was superior to the BTT
costs, and DALYs was larger than the incremental strategy in terms of averting more renal disease and
differences made by these slight adjustments to the BTT ulcer complications when insulin was unavailable (by
microvascular treatment threshold. Hence, the overall 300–368 events per 100 000 people with diabetes).
effectiveness and cost-effectiveness under these However, the BTT strategy remained significantly more
alternative treatment thresholds (3% or 7% lifetime risk) cost-effective than the TTT strategy relative to the no
largely overlapped with those of the base case (5%), with treatment scenario because of the higher number of
the BTT strategy remaining significantly better than the cardiovascular events prevented (by 1800–2100 events per
TTT strategy even after accounting for uncertainties in 100 000 people with diabetes), which outweighed the
risk calculation and input parameter values through the smaller difference in microvascular events prevented.
discrete sensitivity analysis. The proportion of major microvascular events prevented
The use of fasting plasma glucose (target <7 mmol/L)28 decreased by as much as 40% because of the unavailability
rather than HbA1c to guide TTT treatment had no major of insulin, and overall costs increased because the high
www.thelancet.com/diabetes-endocrinology Vol 4 November 2016 927
Articles
China Ghana India Mexico South Africa
People prevented from a complication by both TTT and BTT
Number of people, per 100 000 people with 3183·5 (79·0) 3301·3 (70·4) 3547·9 (64·7) 3252·2 (67·8) 3239·8 (73·9)
type 2 diabetes
Absolute number of people 2 902 000 (72 000) 11 000 (1000) 2 388 000 (44 000) 401 000 (8000) 79 000 (2000)
Age, years 56·4 (2·2) 56·4 (1·2) 56·4 (2·0) 56·5 (2·6) 56·6 (2·3)
Female sex 56·0% (11·2) 56·2% (6·7) 56·6% (11·3) 55·9% (8·9) 55·9% (8·9)
Systolic blood pressure, mm Hg 144·2 (2·9) 151·5 (3·1) 133·9 (2·4) 144·2 (2·2) 143·4 (2·3)
LDL, mmol/L 3·1 (0·1) 3·2 (0·1) 3·3 (0·2) 3·2 (0·1) 3·2 (0·1)
HbA1c 8·6% (0·4) 9·2% (0·2) 8·8% (0·4) 9·5% (0·4) 9·2% (0·2)
Current tobacco smokers, both sexes 33·0% (4·7) 9·2% (3·0) 37·4% (5·4) 24·3% (4·4) 27·5% (4·6)
10 year cardiovascular disease risk 27·7% (3·3) 26·3% (3·5) 28·4% (2·8) 27·5% (3·6) 27·8% (3·6)
Lifetime microvascular risk 18·4% (1·3) 19·1% (2·5) 21·1% (3·2) 17·4% (3·1) 16·6% (3·1)
People prevented from a complication by TTT but not BTT
Number of people, per 100 000 people with 2030·9 (50·4) 2129·9 (45·4) 2229·4 (40·7) 2117·6 (44·1) 2126·7 (48·5)
type 2 diabetes
Absolute number of people 1 851 000 (46 000) 7000 (1000) 1 500 000 (27 000) 261 000 (5000) 52 000 (1000)
Age, years 51·3 (1·9) 51·4 (2·1) 51·3 (2·5) 51·2 (1·3) 51·0 (2·3)
Female sex 77·3% (7·4) 77·4% (5·5) 77·6% (5·3) 77·3% (4·2) 77·5% (7·4)
Systolic blood pressure, mm Hg 138·1 (3·0) 145·2 (3·5) 128·1 (3·3) 138·2 (3·2) 137·5 (2·3)
LDL, mmol/L 3·0 (0·2) 3·1 (0·2) 3·1 (0·2) 3·1 (0·1) 3·1 (0·1)
HbA1c 8·2% (0·5) 8·7% (0·4) 8·4% (0·5) 9·0% (0·4) 8·7% (0·5)
Current tobacco smokers, both sexes 32·2% (3·0) 9·1% (1·9) 36·9% (3·4) 24·2% (2·9) 27·1% (3·0)
10 year cardiovascular disease risk 16·9% (2·3) 16·1% (2·1) 17·3% (1·2) 16·7% (1·9) 16·8% (1·6)
Lifetime microvascular risk 11·0% (0·6) 11·4% (1·4) 12·5% (1·2) 10·5% (1·7) 10·1% (1·3)
People prevented from a complication by BTT but not TTT
Number of people, per 100 000 people with 4322·4 (100·3) 3880·5 (70·7) 4430·7 (92·6) 4161·5 (84·8) 4253·2 (88·9)
type 2 diabetes
Absolute number of people 3 941 000 (914 000) 13 000 (2000) 2 982 000 (623 000) 514 000 (105 000) 103 000 (22 000)
Age, years 57·5 (8·6) 57·3 (11·7) 57·1 (6·9) 57·5 (7·1) 57·7 (12·0)
Female sex 57·4% (4·1) 57·6% (4·6) 59·0% (2·3) 57·1% (5·5) 57·0% (5·3)
Systolic blood pressure, mm Hg 134·0 (3·2) 139·7 (3·9) 123·7 (3·6) 133·4 (3·5) 132·7 (3·1)
LDL, mmol/L 2·7 (0·3) 2·8 (0·1) 2·9 (0·2) 2·8 (0·1) 2·8 (0·2)
HbA1c 7·6% (0·4) 8·1% (0·5) 7·8% (0·4) 8·3% (0·5) 8·1% (0·4)
Current tobacco smokers, both sexes 32·8% (6·4) 9·0% (3·5) 37·3% (6·8) 24·6% (5·8) 27·6% (6·0)
10 year cardiovascular disease risk 21·0% (7·1) 19·7% (9·1) 21·1% (5·2) 20·7% (12·1) 21·0% (12·7)
Lifetime microvascular risk 15·5% (6·2) 16·0% (5·6) 17·7% (10·7) 14·6% (4·3) 13·9% (7·1)
Data are mean (SD). TTT=treat-to-target. BTT=benefit-based tailored treatment.
Table 3: Pre-treatment characteristics of patients prevented from a diabetes complication by TTT and BTT strategies
cost of treating preventable complications exceeded the TTT approach compared with the no treatment scenario.
cost of insulin and supplies, leading to a rise in mean We estimated that adherence would need to be 45% lower
cost per DALY averted of $292 for the TTT approach and for BTT than TTT overall for the TTT strategy to become
$1048 for the BTT approach above the base case superior in effectiveness, and 30% lower overall for TTT to
simulation. The BTT strategy was no longer cost saving become superior in cost-effectiveness.
compared with the TTT strategy, but the incremental The combination of the BTT approach for preventing
cost-effectiveness ratio of switching from TTT to BTT cardiovascular complications with the TTT approach for
varied from $840 to $1600 per DALY averted and was less preventing microvascular complications (appendix
than the gross domestic product per person in all pp 27–28) would have intermediate effectiveness
countries modelled.18 compared with either approach, with less synergistic
If a BTT guideline had a 10% lower adherence from prevention of cardiovascular events through averting
practitioners than had the TTT approach (appendix microvascular disease (eg, cardiovascular events
pp 25–26), this strategy would still avert more cardiovascular prevented by preventing kidney disease) than when
and microvascular complications at a population level, and adopting BTT for both cardiovascular and microvascular
maintain a lower mean cost-effectiveness ratio than the disease prevention. Compared with the use of the BTT
928 www.thelancet.com/diabetes-endocrinology Vol 4 November 2016
Articles
strategy for both cardiovascular and microvascular was fundamentally unable to consistently direct therapy
disease prevention, the number of myocardial infarctions towards individuals who would most benefit. However,
and strokes prevented by the combination approach was the superiority of the BTT strategy for preventing
reduced by roughly 4% and the number of blindness and microvascular events might crucially depend on the
renal disease complications prevented was reduced by availability of insulin, which is not always accessible in
about 3%, with no significant change in ulcer outcomes. some low-income and middle-income countries. The
TTT strategy would be superior to the BTT strategy if
Discussion insulin were unavailable, in terms of preventing end-
We found that a strategy focused on reaching target levels stage renal disease and blindness. Nevertheless, the BTT
of biomarkers (ie, a TTT strategy) would be expected to strategy remained more effective overall because it could
avert 24–31% fewer complications of diabetes than would avert five times more cardiovascular complications and
a strategy focused on treating individuals with a high was therefore more cost-effective than the TTT strategy
estimated risk of complications (ie, a BTT strategy). The even in the absence of insulin. Overall, glycaemic control
TTT strategy was more costly and less effective with insulin adds substantially to the complexities of
($3100–5500 more expensive per DALY averted), and less patient care and to the logistics and cost of drug
efficient in terms of DALYs averted per dollar and DALYs purchasing and distribution.43
averted per 1000 patient-years of medication. Because of Our analysis benefited from the use of equations that
complex interactions between microvascular and have been validated in ethnically diverse populations,25,26
cardiovascular events (eg, renal disease modifies the risk data from recent nationally representative WHO
of cardiovascular complications), treatment to reduce surveys providing consistent measurements of
microvascular risk also affected cardiovascular outcomes, biomarkers,21 and meta-analyses of international trials
which accentuated the superiority of the BTT strategy to inform estimates of relative risk reduction rather
compared with the TTT strategy. The TTT approach was than assuming reversibility of risk. However, the
particularly inferior because the risk of any given diabetes analysis had several important limitations. We had to
complication was based on multiple simultaneous factors assume that UKPDS equations would be relevant and
rather than any single biomarker; hence, the TTT strategy capture risks in populations of the countries studied,
China Ghana India Mexico South Africa
People treated with more medications by TTT
Proportion of people with type 2 26·8% (0·2) 32·6% (0·2) 28·1% (0·3) 29·2% (0·2) 28·4% (0·2)
diabetes
Absolute number of people 24 432 000 (182 000) 111 000 (1000) 18 912 000 (202 000) 3 604 000 (25 000) 688 000 (5000)
Age, years 56·3 (9·8) 59·8 (6·7) 59·7 (6·6) 59·7 (6·6) 59·8 (6·6)
Female sex 85·1% (6·3) 85·3% (3·6) 85·1% (3·2) 84·8% (3·3) 85·7% (5·8)
Current tobacco smokers, both sexes 16·7% (3·0) 3·6% (1·3) 20·2% (2·8) 11·4% (2·1) 13·1% (2·3)
Systolic blood pressure, mm Hg
Initial 146·6 (11·3) 153·7 (12) 136·4 (13·7) 146·5 (9·5) 145·7 (14·4)
Final 129·9 (8·3) 129·9 (8·3) 129·9 (8·3) 129·9 (8·3) 129·9 (8·3)
LDL, mmol/L
Initial 3·1 (0·4) 3·2 (0·5) 3·3 (0·4) 3·2 (0·4) 3·2 (0·3)
Final 2·6 (0·4) 2·6 (0·4) 2·6 (0·4) 2·6 (0·4) 2·6 (0·4)
HbA1c
Initial 7·8% (0·5) 8·3% (0·7) 8·0% (0· 6) 8·6% (0·4) 8·3% (0·7)
Final 6·9% (0·5) 6·9% (0·5) 6·9% (0·5) 6·9% (0·5) 6·9% (0·5)
10 year cardiovascular disease risk
Initial 12·3% (7·0) 12·5% (6·4) 13·3% (4·5) 12·6% (4·2) 12·7% (5·5)
Final 7·8% (3·7) 7·7% (3·4) 8·2% (2·3) 7·8% (2·5) 7·9% (2·8)
Lifetime microvascular risk
Initial 15·0% (7·2) 16·0% (8·2) 18·1% (10·4) 14·0% (5·8) 13·0% (6·9)
Final 13·5% (6·2) 14·4% (7·4) 16·3% (7·9) 12·6% (5·9) 11·6% (5·8)
Cost-effectiveness ratio in treated $20 029·0 (1079·0) $38 800·8 (1461·4) $30 698·0 (1815·4) $21 183·4 (708·3) $45 026·1 (2744·6)
population, per DALY averted
DALYs averted per 1000 patient- 2·8 (6·4) 1·3 (2·4) 2·0 (2·3) 2·9 (4·0) 1·0 (1·9)
years of medication
(Table 4 continues on next page)
www.thelancet.com/diabetes-endocrinology Vol 4 November 2016 929
Articles
China Ghana India Mexico South Africa
(Continued from previous page)
People treated with more medications by BTT
Proportion of people with type 2 55·5% (0·2) 48·2% (0·2) 52·9% (0·2) 52·1% (0·2) 52·9% (0·1)
diabetes
Absolute number of people 50 597 000 (182 000) 165 000 (1000) 35 602 000 (135 000) 6 430 000 (25 000) 1 282 000 (2000)
Age, years 59·6 (6·6) 54·1 (11·5) 54·1 (10·4) 54·7 (10·7) 53·9 (10·8)
Female sex 31·6% (8·2) 26·1% (6·7) 31·0% (7·7) 26·4% (7·3) 34·1% (7·8)
Current tobacco smokers, both sexes 42·7% (6·8) 13·8% (4·2) 44·9% (7·0) 26·1% (5·8) 36·9% (6·5)
Systolic blood pressure, mm Hg
Initial 137·9 (8·5) 144·5 (12·0) 127·8 (8·4) 137·7 (9·0) 136·9 (7·8)
Final 115·7 (7·1) 121·7 (9·8) 107·1 (11·5) 115·7 (8·0) 115 (8·3)
LDL, mmol/L
Initial 2·9 (0·4) 3·0 (0·4) 3·1 (0·4) 3·0 (0·5) 3·0 (0·3)
Final 2·1 (0·4) 2·2 (0·4) 2·2 (0·4) 2·2 (0·5) 2·2 (0·2)
HbA1c
Initial 8·7% (0·9) 9·3% (1·0) 8·9% (1·2) 9·5% (1·5) 9·3% (1·0)
Final 6·8% (0·6) 7·1% (1·0) 6·9% (1·1) 7·4% (0·8) 7·2% (0·8)
10 year cardiovascular disease risk
Initial 24·9% (13·0) 24·5% (8·5) 25·8% (7·9) 25·0% (9·3) 25·1% (20·0)
Final 13·1% (6·5) 12·9% (4·0) 13·5% (3·4) 13·1% (4·6) 13·2% (9·7)
Lifetime microvascular risk
Initial 17·9% (9·5) 18·8% (13·6) 20·9% (12·8) 16·8% (10·3) 15·7% (16·2)
Final 13·5% (7·0) 13·8% (9·8) 15·8% (10·0) 12·4% (10·2) 11·4% (9·3)
Cost-effectiveness ratio in treated $7892·8 (198·7) $12 343·8 (505·3) $11 402·6 (220·8) $8336·6 (192·2) $12 039·4 (289·6)
population, per DALY averted
DALYs averted per 1000 patient- 3·3 (8·5) 1·6 (5·8) 2·3 (3·9) 3·4 (6·0) 1·2 (2·5)
years of medication
Data are mean (SD). Costs are in 2016 US dollars. TTT=treat-to-target. BTT=benefit-based tailored treatment. DALY=disability-adjusted life-year.
Table 4: Comparison of patients treated more intensively (ie, with more medications) by TTT or BTT strategies for reducing complications of type 2 diabetes
using ethnicity-specific parameters that capture require further investigation: the BTT approach to
variations in risk in people of African and south Asian glycaemic control has not been directly studied in
descent. Similar parameters were unavailable for the clinical trials, and this is the necessary next step in
Chinese population, and whether this population would research after this comparative effectiveness modelling
have substantial variations in risk equations remains study. Compared with the TTT approach, the risk of
unclear. However, the availability of more population- hypoglycaemia might be higher under the BTT strategy
specific parameters is unlikely to alter the comparative because more insulin treatment is recommended at a
benefits of the two strategies. Moreover, we did not population level. We also focused on medications
have data on access or adherence to therapy, which available on the WHO Essential Medicines list, which
would linearly scale our results to lower impact; hence, might be expanded pending cost-effectiveness
we focused on how different guidelines would offer assessments of new agents. Statins might also become
different treatment recommendations, and estimated more accessible, and our estimates of cardiovascular
the (large) degree to which adherence would have to be event outcomes would be subject to an additional
differentially worse in the BTT scenario to neutralise 14% relative risk reduction if simvastatin 40 mg daily
our finding of superior outcomes of the BTT approach. were replaced by atorvastatin 40 mg daily,34 further
We found that the superiority of BTT to TTT was increasing the effectiveness of the BTT approach over
consistent for settings in which HbA1c testing was the TTT approach.
unavailable, but further work would need to determine In future work, researchers should also examine how
what strategy would be optimal in settings without importantly risk equation coefficients vary among diverse
insulin access. Importantly, we did not have data on cohorts, and how both patients and clinicians in diverse
differential risk of hypoglycaemia and other adverse settings respond to the prospect of shifting towards a
events with the two approaches, or data on detailed BTT approach to therapy. Our results highlight the
treatment availability and quality. These issues will importance of further data collection for individual
930 www.thelancet.com/diabetes-endocrinology Vol 4 November 2016
Articles
countries to determine optimal and cost-effective risk 16 Stratton IM, Cull CA, Adler AI, Matthews DR, Neil HAW,
Holman RR. Additive effects of glycaemia and blood pressure
thresholds for therapy, as has occurred for statin therapy exposure on risk of complications in type 2 diabetes: a prospective
in people without diabetes in some high-income observational study (UKPDS 75). Diabetologia 2006; 49: 1761–69.
countries.44 Before such work is undertaken, our results 17 Basu S, Bendavid E, Sood N. Health and economic implications of
indicate that a BTT strategy would be more effective and national treatment coverage for cardiovascular disease in india
cost-effectiveness analysis. Circ Cardiovasc Qual Outcomes 2015;
cost-effective than a TTT strategy overall, primarily by 8: 541–51.
concentrating effective therapy in patients with a high 18 World Bank. World development indicators 2014. Washington, DC:
risk of cardiovascular and microvascular complications. World Bank Publications, 2015.
19 UN. World population prospects: the 2012 revision. Geneva:
Contributors United Nations, 2013.
JSY conceived the study and edited the report. VS programmed the 20 International Diabetes Federation. Diabetes atlas. Brussels:
base code. SB revised the code, implemented the analysis, and drafted International Diabetes Federation, 2015.
the report. 21 Kowal P, Chatterji S, Naidoo N, et al. Data resource profile:
Declaration of interests the World Health Organization Study on global AGEing and adult
health (SAGE). Int J Epidemiol 2012; 41: 1639–49.
We declare no competing interests.
22 Public Health England. Adult obesity and type 2 diabetes.
Acknowledgments London: Public Health England. https://www.gov.uk/government/
Data for this project were obtained from the WHO Study on Global publications/adult-obesity-and-type-2-diabetes (accessed
Aging and Adult Health (SAGE), which is supported by the US National Aug 23, 2016).
Institute on Aging’s Division of Behavioral and Social Research through 23 Menke A, Casagrande S, Geiss L, Cowie CC. Prevalence of and
interagency agreements and research grants (R01 AG034479) and by the trends in diabetes among adults in the United States, 1988–2012.
WHO’s Department of Health Statistics and Information Systems. JAMA 2015; 314: 1021–29.
24 Guariguata L, Whiting DR, Hambleton I, Beagley J, Linnenkamp U,
References Shaw JE. Global estimates of diabetes prevalence for 2013 and
1 Global Burden of Disease Study 2013 Collaborators. projections for 2035. Diabetes Res Clin Pract 2014; 103: 137–49.
Global, regional, and national incidence, prevalence, and years lived
25 Hayes AJ, Leal J, Gray AM, Holman RR, Clarke PM.
with disability for 301 acute and chronic diseases and injuries in
UKPDS outcomes model 2: a new version of a model to simulate
188 countries, 1990–2013: a systematic analysis for the Global
lifetime health outcomes of patients with type 2 diabetes mellitus
Burden of Disease Study 2013. Lancet 2015; 386: 743–800.
using data from the 30 year United Kingdom Prospective Diabetes
2 Tight blood pressure control and risk of macrovascular and Study: UKPDS 82. Diabetologia 2013; 56: 1925–33.
microvascular complications in type 2 diabetes: UKPDS 38.
26 Clarke P. Constructing diabetes model from individual level data.
UK Prospective Diabetes Study Group. BMJ 1998; 317: 703–13.
Palo Alto: Stanford University, 2014.
3 Zoungas S, Chalmers J, Neal B, et al. Follow-up of blood-pressure
27 American Diabetes Association. Dyslipidemia management in
lowering and glucose control in type 2 diabetes. N Engl J Med 2014;
adults with diabetes. Diabetes Care 2004; 27: s68–71.
371: 1392–406.
28 WHO. Package of essential noncommunicable (pen) disease
4 Duckworth W, Abraira C, Moritz T, et al. Glucose control and
interventions for primary health care in low-resource settings.
vascular complications in veterans with type 2 diabetes.
Geneva: World Health Organization, 2013.
N Engl J Med 2009; 360: 129–39.
29 Law MR, Wald NJ, Morris JK, Jordan RE. Value of low dose
5 American Diabetes Association. Standards of medical care in
combination treatment with blood pressure lowering drugs:
diabetes—2014. Diabetes Care 2014; 37: S14–80.
analysis of 354 randomised trials. BMJ 2003; 326: 1427.
6 Goff DC, Lloyd-Jones DM, Bennett G, et al. 2013 ACC/AHA
30 Law MR, Wald NJ, Rudnicka AR. Quantifying effect of statins on
guideline on the assessment of cardiovascular risk.
low density lipoprotein cholesterol, ischaemic heart disease, and
J Am Coll Cardiol 2014; 63: 2935–59.
stroke: systematic review and meta-analysis. BMJ 2003; 326: 1423.
7 Muntner P, Colantonio LD, Cushman M, et al. Validation of the
31 Lewington S, Clarke R, Qizilbash N, Peto R, Collins R,
atherosclerotic cardiovascular disease Pooled Cohort risk equations.
Prospective Studies Collaboration. Age-specific relevance of usual
JAMA 2014; 311: 1406–15.
blood pressure to vascular mortality: a meta-analysis of individual
8 Pandya A, Sy S, Cho S, Weinstein MC, Gaziano TA. data for one million adults in 61 prospective studies. Lancet 2002;
Cost-effectiveness of 10-year risk thresholds for initiation of statin 360: 1903–13.
therapy for primary prevention of cardiovascular disease. JAMA
32 Cholesterol Treatment Trialists’ (CTT) Collaborators. Efficacy and
2015; 314: 142–50.
safety of cholesterol-lowering treatment: prospective meta-analysis
9 Eddy DM, Adler J, Patterson B, Lucas D, Smith KA, Morris M. of data from 90 056 participants in 14 randomised trials of statins.
Individualized guidelines: the potential for increasing quality and Lancet 2005; 366: 1267–78.
reducing costs. Ann Intern Med 2011; 154: 627.
33 Hemmingsen B, Lund SS, Gluud C, et al. Targeting intensive
10 Sussman J, Vijan S, Hayward R. Using benefit-based tailored glycaemic control versus targeting conventional glycaemic control
treatment to improve the use of antihypertensive medications. for type 2 diabetes mellitus. Cochrane Database Syst Rev 2011;
Circulation 2013; 128: 2309–17. 6: CD008143.
11 SPRINT Research Group, Wright JT, Williamson JD, et al. 34 Hayward RA, Krumholz HM, Zulman DM, Timbie JW, Vijan S.
A randomized trial of intensive versus standard blood-pressure Optimizing statin treatment for primary prevention of coronary
control. N Engl J Med 2015; 373: 2103–16. artery disease. Ann Intern Med 2010; 152: 69–77.
12 Lonn EM, Bosch J, López-Jaramillo P, et al. Blood-pressure lowering 35 Basu S, Yudkin JS, Sussman JB, Millett C, Hayward RA.
in intermediate-risk persons without cardiovascular disease. Alternative strategies to achieve cardiovascular mortality goals in
N Engl J Med 2016; 374: 2009–20. China and India: a microsimulation of target- versus risk-based
13 The Blood Pressure Lowering Treatment Trialists’ Collaboration. blood pressure treatment. Circulation 2016; 133: 840–48.
Blood pressure-lowering treatment based on cardiovascular risk: 36 Mendis S, Fukino K, Cameron A, et al. The availability and
a meta-analysis of individual patient data. Lancet 2014; 384: 591–98. affordability of selected essential medicines for chronic diseases in
14 The Action to Control Cardiovascular Risk in Diabetes Study Group. six low- and middle-income countries. Bull World Health Organ
Effects of intensive glucose lowering in type 2 diabetes. 2007; 85: 279–88.
N Engl J Med 2008; 358: 2545–59. 37 WHO. WHO model list of essential medicines, 19th edn. Geneva:
15 Boussageon R, Bejan-Angoulvant T, Saadatian-Elahi M, et al. World Health Organization, 2015.
Effect of intensive glucose lowering treatment on all cause mortality, 38 WHO. Choosing interventions that are cost effective
cardiovascular death, and microvascular events in type 2 diabetes: (WHO-CHOICE). Geneva: World Health Organization, 2010.
meta-analysis of randomised controlled trials. BMJ 2011; 343: d4169.
www.thelancet.com/diabetes-endocrinology Vol 4 November 2016 931
Articles
39 Husereau D, Drummond M, Petrou S, et al. Consolidated health 42 Management Sciences for Health. International drug price
economic evaluation reporting standards (CHEERS)—explanation indicator guide. Cambridge, MA: Management Sciences for Health,
and elaboration: a report of the ISPOR Health Economic Evaluation 2015 http://www.msh.org/sites/msh.org/files/international-drug-
Publication Guidelines Good Reporting Practices Task Force. price-indicator-guide.pdf (accessed Jan 28, 2015).
Value Health 2013; 16: 231–50. 43 Beran D, Ewen M, Laing R. Constraints and challenges in access to
40 Danaei G, Finucane MM, Lu Y, et al. National, regional, and global insulin: a global perspective. Lancet Diabetes Endocrinol 2016;
trends in fasting plasma glucose and diabetes prevalence since 4: 275–85.
1980: systematic analysis of health examination surveys and 44 Pandya A, Sy S, Cho S, Weinstein MC, Gaziano TA.
epidemiological studies with 370 country-years and 2·7 million Cost-effectiveness of 10-year risk thresholds for initiation of statin
participants. Lancet 2011; 378: 31–40. therapy for primary prevention of cardiovascular disease. JAMA
41 Salomon JA, Vos T, Hogan DR, et al. Common values in assessing 2015; 314: 142–50.
health outcomes from disease and injury: disability weights
measurement study for the Global Burden of Disease Study 2010.
Lancet 2013; 380: 2129–43.
932 www.thelancet.com/diabetes-endocrinology Vol 4 November 2016
Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Diet Review 39 Popular Nutrition and Weight Loss Plans and The Science or Lack of Science Behind Them Harvard HealthДокумент57 страницThe Diet Review 39 Popular Nutrition and Weight Loss Plans and The Science or Lack of Science Behind Them Harvard HealthJohnny92% (12)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- 101 Juice Recipes - Cross, JoeДокумент478 страниц101 Juice Recipes - Cross, JoeShivam Patel94% (82)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Ingles Parcial Domiciliario 2022Документ5 страницIngles Parcial Domiciliario 2022Macarena zapattaОценок пока нет
- Too Many Pills - How Too Much Me - James Le FanuДокумент274 страницыToo Many Pills - How Too Much Me - James Le Fanumohamed gaberОценок пока нет
- SSSL Checklist FinalJun08Документ1 страницаSSSL Checklist FinalJun08Ari AzhariОценок пока нет
- Ramseysedationscale PDFДокумент1 страницаRamseysedationscale PDFAri AzhariОценок пока нет
- WHO Safe Childbirth Checklist: On AdmissionДокумент4 страницыWHO Safe Childbirth Checklist: On AdmissionAri AzhariОценок пока нет
- Nancy Kamau PDFДокумент47 страницNancy Kamau PDFAri Azhari100% (1)
- Nurse Work Motivation TransletДокумент107 страницNurse Work Motivation TransletAri AzhariОценок пока нет
- Nurse Work Motivation TransletДокумент107 страницNurse Work Motivation TransletAri AzhariОценок пока нет
- Motivatoin and LeadershipДокумент47 страницMotivatoin and LeadershipAri AzhariОценок пока нет
- Documentation 1.en - IdДокумент2 страницыDocumentation 1.en - IdAri AzhariОценок пока нет
- Motivatoin and LeadershipДокумент12 страницMotivatoin and LeadershipAri AzhariОценок пока нет
- Motivation 1.en - IdДокумент10 страницMotivation 1.en - IdAri AzhariОценок пока нет
- Documentation 1.en - Id 1Документ2 страницыDocumentation 1.en - Id 1Ari AzhariОценок пока нет
- Motivation and Leadership TransletДокумент11 страницMotivation and Leadership TransletAri AzhariОценок пока нет
- Sebuah Grup Kunjungi Initiative Meningkatkan Muka Perencanaan Perawatan Dokumentasi Antara Dewasa Lama Di Primary CareДокумент11 страницSebuah Grup Kunjungi Initiative Meningkatkan Muka Perencanaan Perawatan Dokumentasi Antara Dewasa Lama Di Primary CareAri AzhariОценок пока нет
- A Group Visit Initiative Improves Advance Care Planning Documentation Among Older Adults in Primary CareДокумент11 страницA Group Visit Initiative Improves Advance Care Planning Documentation Among Older Adults in Primary CareAri AzhariОценок пока нет
- Gambaran Self Care Penderita Diabetes Melitus (DM) Di Wilayah Kerja Puskesmas Srondol SemarangДокумент8 страницGambaran Self Care Penderita Diabetes Melitus (DM) Di Wilayah Kerja Puskesmas Srondol SemarangAri AzhariОценок пока нет
- (CPG) Philippine Guidelines On Periodic Health Examination: Lifestyle AdviceДокумент107 страниц(CPG) Philippine Guidelines On Periodic Health Examination: Lifestyle AdviceBianca Watanabe - RatillaОценок пока нет
- q1 Hope 3 Module 1Документ16 страницq1 Hope 3 Module 1Dianara SongcuyaОценок пока нет
- A Comprehensive Review On Metabolic SyndromeДокумент36 страницA Comprehensive Review On Metabolic SyndromekotraeОценок пока нет
- Evaluacion Pulmonar PreoperatoriaДокумент15 страницEvaluacion Pulmonar Preoperatorialuis castillejosОценок пока нет
- Presentation On WalnutДокумент5 страницPresentation On WalnutSheikh JeelaniОценок пока нет
- 500-ALPHA FIT Testers ManualДокумент29 страниц500-ALPHA FIT Testers ManualDarío Gerpe MeirásОценок пока нет
- Aon - Global Medical Trend Rate Survey Report 2013 2014Документ22 страницыAon - Global Medical Trend Rate Survey Report 2013 2014Jerome GelfandОценок пока нет
- The Secrets of LongevityДокумент11 страницThe Secrets of Longevitycarly183100% (10)
- 23-5-2022 Presentation JentadeutoДокумент52 страницы23-5-2022 Presentation JentadeutofsvtqsОценок пока нет
- (World Review of Nutrition and Dietetics) Simopoulos A. (Ed.) - Nutrition and Fitness-Karger (2008) PDFДокумент326 страниц(World Review of Nutrition and Dietetics) Simopoulos A. (Ed.) - Nutrition and Fitness-Karger (2008) PDFNoemiKissОценок пока нет
- Brief History and Nature of DanceДокумент25 страницBrief History and Nature of Dancewelmar laordenОценок пока нет
- Cardiac Diet PlanДокумент8 страницCardiac Diet PlanCosma MonicaОценок пока нет
- Lipids (Mcmurry Ch. 27)Документ15 страницLipids (Mcmurry Ch. 27)Meisy RadhistaОценок пока нет
- First Summative TestДокумент2 страницыFirst Summative TestMaan BautistaОценок пока нет
- Vision and AgeingДокумент421 страницаVision and AgeingFaheem KvОценок пока нет
- Summary Notes - Topic 1 Edexcel (A) Biology A LevelДокумент10 страницSummary Notes - Topic 1 Edexcel (A) Biology A LevelAmal Abu KhalilОценок пока нет
- RSO Service DirectoryДокумент5 страницRSO Service Directorydebbie_simОценок пока нет
- 1432.full 2Документ10 страниц1432.full 2Gokull ShautriОценок пока нет
- Hypertension in ElderlyДокумент13 страницHypertension in ElderlybookwormMD100% (2)
- AppleДокумент13 страницAppleAyishaОценок пока нет
- Long-Term Risks of Vasectomy - GLOWMДокумент53 страницыLong-Term Risks of Vasectomy - GLOWMLila Tri HarjanaОценок пока нет
- Edexcel Biology Unit 1 AS FlashcardsДокумент42 страницыEdexcel Biology Unit 1 AS FlashcardsBodayaОценок пока нет
- Please Search On The Filipino Cultural Characteristics and Health Care Beliefs and Practices in Health EducationДокумент16 страницPlease Search On The Filipino Cultural Characteristics and Health Care Beliefs and Practices in Health Educationthe someoneОценок пока нет
- ACC166 Assignment 9Документ5 страницACC166 Assignment 9URANG CHITOОценок пока нет
- Ade Egie Prayogi - Perbaikan InggrisДокумент6 страницAde Egie Prayogi - Perbaikan InggrisAde Egie PrayogiОценок пока нет
- How Obesity Affects Our Health?Документ6 страницHow Obesity Affects Our Health?Mark PadernalОценок пока нет