Вам также может понравиться
- Robert Tibbo - Letter To PM Canada - 3 October 2019 (En - FR)Документ10 страницRobert Tibbo - Letter To PM Canada - 3 October 2019 (En - FR)LeMonde.frОценок пока нет
- 2020.05.07 Commission EU Proposition de Classification Du SARS-CoV-2Документ11 страниц2020.05.07 Commission EU Proposition de Classification Du SARS-CoV-2LeMonde.frОценок пока нет
- Position Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019Документ8 страницPosition Paper de l'UEFA Sur L'interdiction Du Gazon Synthétique Par l'ECHA 19 Juillet 2019LeMonde.frОценок пока нет
- 2019.08.23 Fieldfisher Letter PDFДокумент10 страниц2019.08.23 Fieldfisher Letter PDFLeMonde.frОценок пока нет
- Robert Tibbo - Letter To PM Canada - 3 October 2019 (En - FR)Документ10 страницRobert Tibbo - Letter To PM Canada - 3 October 2019 (En - FR)LeMonde.frОценок пока нет
- Rapport NCAR Envoyé Par La France Sur Les Incidents Concernant Les Implants Mammaires PIP en 2010.Документ2 страницыRapport NCAR Envoyé Par La France Sur Les Incidents Concernant Les Implants Mammaires PIP en 2010.LeMonde.frОценок пока нет
- 7 Mars 2019 Note de La DG Santé Au Chef de Cabinet Du Commissaire Européen À La SantéДокумент4 страницы7 Mars 2019 Note de La DG Santé Au Chef de Cabinet Du Commissaire Européen À La SantéLeMonde.fr100% (1)
- 2013.09.13 Eucomed. Lettre Au Commissaire Neven MimicaДокумент1 страница2013.09.13 Eucomed. Lettre Au Commissaire Neven MimicaLeMonde.frОценок пока нет
- 1er Février 2012. Commission Européenne PIP "Stress Test".Документ15 страниц1er Février 2012. Commission Européenne PIP "Stress Test".LeMonde.frОценок пока нет
- Gender Pay Gap Tech Report 2018Документ8 страницGender Pay Gap Tech Report 2018LeMonde.frОценок пока нет
- Echanges Sur La Mission Et Le Tarif de David KirklandДокумент12 страницEchanges Sur La Mission Et Le Tarif de David KirklandLeMonde.frОценок пока нет
- Monsanto Estime Jess Rowland "Utile"Документ1 страницаMonsanto Estime Jess Rowland "Utile"LeMonde.frОценок пока нет
- Jess Rowland Demande Une MédailleДокумент4 страницыJess Rowland Demande Une MédailleLeMonde.frОценок пока нет
- 6 Février 2012 TEAM-NB Sujet: Position Des Organismes Notifiés Sur La Surveillance Et L'examen Des Implants À Haut RisqueДокумент3 страницы6 Février 2012 TEAM-NB Sujet: Position Des Organismes Notifiés Sur La Surveillance Et L'examen Des Implants À Haut RisqueLeMonde.frОценок пока нет
- Lettre de Christopher Portier À Jean-Claude Juncker Du 28 Mai 2017Документ8 страницLettre de Christopher Portier À Jean-Claude Juncker Du 28 Mai 2017LeMonde.frОценок пока нет
- Echanges Entre William Heydens de Monsanto Et John AcquavellaДокумент7 страницEchanges Entre William Heydens de Monsanto Et John AcquavellaLeMonde.frОценок пока нет
- Echanges de Monsanto Sur La Constitution D'un Panel GlyphosateДокумент7 страницEchanges de Monsanto Sur La Constitution D'un Panel GlyphosateLeMonde.frОценок пока нет
- Contrat de Consultant de A. Wallace Hayes Avec MonsantoДокумент1 страницаContrat de Consultant de A. Wallace Hayes Avec MonsantoLeMonde.frОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- High-Definition Multimedia Interface SpecificationДокумент51 страницаHigh-Definition Multimedia Interface SpecificationwadrОценок пока нет
- Consolidated Digests - Part 2Документ314 страницConsolidated Digests - Part 2Neil Patrick Pepito ErmacОценок пока нет
- International Economics 16Th Edition Thomas Pugel Test Bank Full Chapter PDFДокумент45 страницInternational Economics 16Th Edition Thomas Pugel Test Bank Full Chapter PDFRebeccaBartlettqfam100% (11)
- Man 3Документ38 страницMan 3Paylo KatolykОценок пока нет
- Soal TKM B. Inggris Kls XII Des. 2013Документ8 страницSoal TKM B. Inggris Kls XII Des. 2013Sinta SilviaОценок пока нет
- Lesson For SpreadsheetsДокумент69 страницLesson For SpreadsheetsCrisna Rivera PundanoОценок пока нет
- BON Resolution No 08 1994Документ2 страницыBON Resolution No 08 1994Noel100% (9)
- Security Enhancement in 2016 SQL ServerДокумент21 страницаSecurity Enhancement in 2016 SQL ServerAtul SharmaОценок пока нет
- Tesco Travel Policy BookletДокумент64 страницыTesco Travel Policy Bookletuser001hОценок пока нет
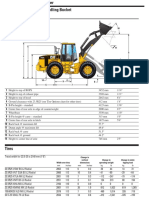
- Cat It62hДокумент4 страницыCat It62hMarceloОценок пока нет
- Oxford Handbooks Online: From Old To New Developmentalism in Latin AmericaДокумент27 страницOxford Handbooks Online: From Old To New Developmentalism in Latin AmericadiegoОценок пока нет
- People/Occupancy Rules of Thumb: Bell - Ch10.indd 93 8/17/07 10:39:31 AMДокумент8 страницPeople/Occupancy Rules of Thumb: Bell - Ch10.indd 93 8/17/07 10:39:31 AMPola OsamaОценок пока нет
- Transformative Change at PPLДокумент24 страницыTransformative Change at PPLAli A. KhokhArОценок пока нет
- Beijing-Michael PageДокумент71 страницаBeijing-Michael Pagejohndavsg8022Оценок пока нет
- PLLV Client Consent FormДокумент4 страницыPLLV Client Consent Formapi-237715517Оценок пока нет
- CV Rafi Cargill, GAR, MCR, AM GROUP and Consultancy EraДокумент6 страницCV Rafi Cargill, GAR, MCR, AM GROUP and Consultancy EranorulainkОценок пока нет
- U-Blox Parameters Setting ProtocolsДокумент2 страницыU-Blox Parameters Setting Protocolspedrito perezОценок пока нет
- Guest AccountingДокумент8 страницGuest Accountingjhen01gongonОценок пока нет
- Rectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadДокумент3 страницыRectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadbashaОценок пока нет
- News/procurement-News: WWW - Sbi.co - inДокумент15 страницNews/procurement-News: WWW - Sbi.co - inssat111Оценок пока нет
- Introduction To GlobalizationДокумент17 страницIntroduction To Globalization21100959Оценок пока нет
- COST v. MMWD Complaint 8.20.19Документ64 страницыCOST v. MMWD Complaint 8.20.19Will HoustonОценок пока нет
- 06 BuyLog2013 MoldedCaseCircBrkrsДокумент106 страниц06 BuyLog2013 MoldedCaseCircBrkrsmarbyОценок пока нет
- In Coming MailДокумент4 страницыIn Coming Mailpoetoet100% (1)
- IM0973567 Orlaco EMOS Photonview Configuration EN A01 MailДокумент14 страницIM0973567 Orlaco EMOS Photonview Configuration EN A01 Maildumass27Оценок пока нет
- Sampling PowerpointДокумент21 страницаSampling PowerpointMuhammad Furqan Aslam AwanОценок пока нет
- Fine Fragrances After Shave, Eau de Parfum, Eau de Cologne, Eau de Toilette, Parfume Products (9-08)Документ6 страницFine Fragrances After Shave, Eau de Parfum, Eau de Cologne, Eau de Toilette, Parfume Products (9-08)Mustafa BanafaОценок пока нет
- წყალტუბოს - სპა კურორტის განვითარების გეგმაДокумент16 страницწყალტუბოს - სპა კურორტის განვითარების გეგმაReginfoОценок пока нет
- Data Loss PreventionДокумент20 страницData Loss Preventiondeepak4315Оценок пока нет
- Reaching Different Learning Styles ThrouДокумент29 страницReaching Different Learning Styles ThrouKENNETH HERRERAОценок пока нет