Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Ultrasound Estimated Subcutaneous and Visceral Adipose Tissue Thicknesses and Risk of Pre EclampsiaДокумент8 страницUltrasound Estimated Subcutaneous and Visceral Adipose Tissue Thicknesses and Risk of Pre Eclampsiamember12dОценок пока нет
- Vitamin D Deficiency and Gestational Diabetes Mellitus in Relation To Body Mass IndexДокумент10 страницVitamin D Deficiency and Gestational Diabetes Mellitus in Relation To Body Mass Indexmember12dОценок пока нет
- Patient Recapitulation Delivery Room ReportДокумент2 страницыPatient Recapitulation Delivery Room Reportmember12dОценок пока нет
- Ram Poli Urogin 13.9.21Документ1 страницаRam Poli Urogin 13.9.21member12dОценок пока нет
- Pre-Eclampsia Is A Valuable Opportunity To Diagnose Chronic Kidney Disease - A Multicentre StudyДокумент11 страницPre-Eclampsia Is A Valuable Opportunity To Diagnose Chronic Kidney Disease - A Multicentre Studymember12dОценок пока нет
- Physical Activity and The Occurence of Postpartum Depression - A Systematic ReviewДокумент25 страницPhysical Activity and The Occurence of Postpartum Depression - A Systematic Reviewmember12dОценок пока нет
- Factors Affecting Use of Magnesium Sulphate For Pre-Eclampsia or Eclampsia - A Qualitative Evidence SynthesisДокумент13 страницFactors Affecting Use of Magnesium Sulphate For Pre-Eclampsia or Eclampsia - A Qualitative Evidence Synthesismember12dОценок пока нет
- Steroids, Steroid Associated Substances, and Gestational Diabetes MellitusДокумент18 страницSteroids, Steroid Associated Substances, and Gestational Diabetes Mellitusmember12dОценок пока нет
- Dietary Factors That Affect The Risk of Pre-EclampsiaДокумент16 страницDietary Factors That Affect The Risk of Pre-Eclampsiamember12dОценок пока нет
- Kom-Daily Cot Monday 13.09.21 FixДокумент3 страницыKom-Daily Cot Monday 13.09.21 Fixmember12dОценок пока нет
- Depression Is A Serious Mental Health ProblemДокумент2 страницыDepression Is A Serious Mental Health Problemmember12dОценок пока нет
- Ino Gynecology II Outpatient (13 September 2021)Документ1 страницаIno Gynecology II Outpatient (13 September 2021)member12dОценок пока нет
- Mola Hidatidosa JESДокумент24 страницыMola Hidatidosa JESmember12dОценок пока нет
- TUGAS CRITICAL APRAISAL - 03 - Abi Rafdi - Obstetri Dan GinekologiДокумент4 страницыTUGAS CRITICAL APRAISAL - 03 - Abi Rafdi - Obstetri Dan Ginekologimember12dОценок пока нет
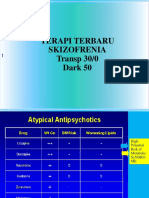
- Terapi Terbaru Skizofrenia Transp 30/0 Dark 50Документ58 страницTerapi Terbaru Skizofrenia Transp 30/0 Dark 50member12dОценок пока нет
- Pregnancy Infection Guide: TORCH PathogensДокумент59 страницPregnancy Infection Guide: TORCH Pathogensmember12dОценок пока нет
- One Lung VentilationДокумент2 страницыOne Lung Ventilationmember12dОценок пока нет
- KET JessicaДокумент44 страницыKET Jessicamember12dОценок пока нет
- Daftar PustakaДокумент1 страницаDaftar Pustakamember12dОценок пока нет
- Daftar PustakaДокумент1 страницаDaftar Pustakamember12dОценок пока нет
- Daftar PustakaДокумент1 страницаDaftar Pustakamember12dОценок пока нет
- Baru Metabolisme LipidДокумент14 страницBaru Metabolisme Lipidmember12dОценок пока нет
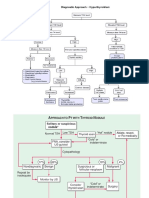
- Diagnostic Approach ThyroidДокумент3 страницыDiagnostic Approach Thyroidmember12dОценок пока нет
- Status Pasien Dengan Keluhan Nyeri BAKДокумент5 страницStatus Pasien Dengan Keluhan Nyeri BAKmember12dОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Mandala Coloring For Children With Symptoms of Attention Deficit Hyperactivity Disorder - A Case SeriesДокумент7 страницMandala Coloring For Children With Symptoms of Attention Deficit Hyperactivity Disorder - A Case Seriesindex PubОценок пока нет
- Sports Injuries ManagementДокумент94 страницыSports Injuries ManagementSaha DirllahОценок пока нет
- Graves DiseaseДокумент7 страницGraves DiseaseNader SmadiОценок пока нет
- CostipitationДокумент4 страницыCostipitationashmi akberОценок пока нет
- Religare Pre Auth FormДокумент3 страницыReligare Pre Auth FormM/s Microtech25% (4)
- Stomach CancerДокумент14 страницStomach CancerLamy SОценок пока нет
- Ketamin FarmakologiДокумент19 страницKetamin FarmakologiBang mantoОценок пока нет
- Chughtai Lab Rate ListДокумент33 страницыChughtai Lab Rate ListHassan Gill67% (9)
- Lina Marulanda - Nursing Resume FinalДокумент2 страницыLina Marulanda - Nursing Resume Finalapi-490969182Оценок пока нет
- Psychoeducation: 19 July 2018 Unit VI Topic DiscussionДокумент26 страницPsychoeducation: 19 July 2018 Unit VI Topic DiscussionDana Franklin100% (1)
- P.E. 1 Module 1 - First Semprelim-MidtermДокумент16 страницP.E. 1 Module 1 - First Semprelim-MidtermLalaine AdtoonОценок пока нет
- Nursing Program Case Analysis FormatДокумент4 страницыNursing Program Case Analysis FormatEmmy Flor ValmoriaОценок пока нет
- UNAIDS Core Epidemiology Slides enДокумент11 страницUNAIDS Core Epidemiology Slides enTabarcea VitaliОценок пока нет
- FFT Neuroma Morton PDFДокумент6 страницFFT Neuroma Morton PDFdasamoroОценок пока нет
- Brain Health Assessment by Dr. Daniel Amen #1 Brain Type QuizДокумент1 страницаBrain Health Assessment by Dr. Daniel Amen #1 Brain Type Quiz03.wizenedwasterОценок пока нет
- Auricular Acupuncture: Prof - Dr.Murugeshbabu, M.SC, M.SC, M.PHIL, M.ACU, M.D, PH.DДокумент74 страницыAuricular Acupuncture: Prof - Dr.Murugeshbabu, M.SC, M.SC, M.PHIL, M.ACU, M.D, PH.DMurugesh BabuОценок пока нет
- EMedicine - Oral Hemangiomas - Article by Steven Brett SloanДокумент19 страницEMedicine - Oral Hemangiomas - Article by Steven Brett SloanDr Monal YuwanatiОценок пока нет
- NBME Answer With Explanation in DepthДокумент10 страницNBME Answer With Explanation in DepthDejan Zolak100% (3)
- High Risk B-Precursor Acute Lymphoblastic Leukemia Interim Maintenance IIДокумент1 страницаHigh Risk B-Precursor Acute Lymphoblastic Leukemia Interim Maintenance IIRitush MadanОценок пока нет
- Global epidemiology of periodontal diseaseДокумент16 страницGlobal epidemiology of periodontal diseaseBrenda Carolina Pattigno ForeroОценок пока нет
- Fi AДокумент67 страницFi AalfonsoОценок пока нет
- OtrivinДокумент12 страницOtrivinkanika sengarОценок пока нет
- Mindworks Testimonials S TitlesДокумент3 страницыMindworks Testimonials S Titlesapi-244257330Оценок пока нет
- Laboratory BacteriologyДокумент39 страницLaboratory BacteriologyDayledaniel SorvetoОценок пока нет
- Ch09 AnaestheticsДокумент21 страницаCh09 AnaestheticsDonna MitchellОценок пока нет
- Coverage Midterm Examination 2021 Drug and Vice ControlДокумент4 страницыCoverage Midterm Examination 2021 Drug and Vice ControlTaga Phase 7Оценок пока нет
- The Microbial World & You: NomenclatureДокумент9 страницThe Microbial World & You: NomenclatureApryll DarlineОценок пока нет
- Cryptogenic StrokeДокумент17 страницCryptogenic StrokeIRENA GENIОценок пока нет
- RADIOLOGYДокумент3 страницыRADIOLOGYwendy carinoОценок пока нет
- Halozyme Therapeutics, Inc. 2009 Investor Day PresentationДокумент88 страницHalozyme Therapeutics, Inc. 2009 Investor Day Presentationsstrumello7395Оценок пока нет