Вам также может понравиться
- Labour Market Economics, 7th Canadian EditionДокумент623 страницыLabour Market Economics, 7th Canadian EditionRitika81% (32)
- 960 C Obs 28 Prevention Detection and Management of Subgaleal Haemorrhage in The NewbornДокумент13 страниц960 C Obs 28 Prevention Detection and Management of Subgaleal Haemorrhage in The NewbornNirubhana ArunthavasothyОценок пока нет
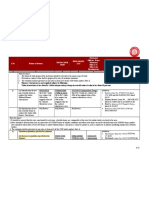
- Amended Formats For Ldce CM 2022Документ73 страницыAmended Formats For Ldce CM 2022K.A.SELVARAJAN AMIEОценок пока нет
- How Inter-Country Differences Affect HRM - 3Документ20 страницHow Inter-Country Differences Affect HRM - 3998621237867% (3)
- Project Report On Jindal Steel & Power Ltd.Документ38 страницProject Report On Jindal Steel & Power Ltd.Gaurav Tripathi71% (7)
- Siig PromoДокумент2 страницыSiig PromobrahmaОценок пока нет
- Dhs Atp 80923Документ14 страницDhs Atp 80923jollanaveen160Оценок пока нет
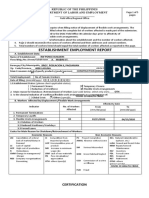
- Establishment Employment ReportДокумент7 страницEstablishment Employment ReportRW Ponce BuildersОценок пока нет
- Phod/Chod /hod Drm/Adrm/ SAG Divisional Officers, Extra Divisional Officers & Officers in Headquarters RemarksДокумент2 страницыPhod/Chod /hod Drm/Adrm/ SAG Divisional Officers, Extra Divisional Officers & Officers in Headquarters Remarkstender cellОценок пока нет
- Basics of Electrical Engineering MaintenanceДокумент57 страницBasics of Electrical Engineering MaintenanceAde ApriОценок пока нет
- Dswd-As-Gf-018 - Rev 03 - Records Disposal RequestДокумент1 страницаDswd-As-Gf-018 - Rev 03 - Records Disposal RequestKim Mark C ParaneОценок пока нет
- RA Document RA Details: GEM/2021/B/1510260Документ2 страницыRA Document RA Details: GEM/2021/B/1510260SITARAM GANESHMALLОценок пока нет
- Establishement Employment ReportДокумент3 страницыEstablishement Employment ReportRW Ponce BuildersОценок пока нет
- PO481Документ6 страницPO481quangthuyqnОценок пока нет
- Draft FCNA Contract # 25-1025-5-1 - 1 (00000004)Документ33 страницыDraft FCNA Contract # 25-1025-5-1 - 1 (00000004)sedew11911Оценок пока нет
- Boat InvoiceДокумент3 страницыBoat InvoiceSairaj PatilОценок пока нет
- TransferДокумент2 страницыTransferRavi KiranОценок пока нет
- Scan Aug 21, 2020Документ1 страницаScan Aug 21, 2020maheshkumarОценок пока нет
- Admission Clearance New Format January 2019Документ1 страницаAdmission Clearance New Format January 2019Le Belle SorianoОценок пока нет
- SS Promotions dt.29.12.2023Документ2 страницыSS Promotions dt.29.12.2023brahmaОценок пока нет
- LOA. 33-11 KV Ss Dhanbad DivДокумент12 страницLOA. 33-11 KV Ss Dhanbad Divsiddhantbmr12Оценок пока нет
- RGC Mint Sheet - ActiveДокумент2 страницыRGC Mint Sheet - ActiverumanzagccОценок пока нет
- Circular - Amendment in Schedule of DPC - 1 and DPC - 2 - 513718 PDFДокумент1 страницаCircular - Amendment in Schedule of DPC - 1 and DPC - 2 - 513718 PDFkhyatichavdaОценок пока нет
- Circular - Amendment in Schedule of DPC - 1 and DPC - 2 - 513718Документ1 страницаCircular - Amendment in Schedule of DPC - 1 and DPC - 2 - 513718khyatichavdaОценок пока нет
- MSOP Part A Item 5 F PDFДокумент3 страницыMSOP Part A Item 5 F PDFHARESH JANIОценок пока нет
- GeM Bidding 6206077Документ7 страницGeM Bidding 6206077nilesh ajmireОценок пока нет
- Organizational Restructuring of MPLS NOCДокумент2 страницыOrganizational Restructuring of MPLS NOCVIKRANTОценок пока нет
- ORDERS 92.1: Edi GuidelineДокумент13 страницORDERS 92.1: Edi GuidelineAlexa MéndezОценок пока нет
- Client Follow Up Report FormДокумент1 страницаClient Follow Up Report FormNicholas Nuwamanya RutaОценок пока нет
- Basics of Electrical Engineering and Maintenance Practices: R. Bhargava / A. R. ShendyeДокумент57 страницBasics of Electrical Engineering and Maintenance Practices: R. Bhargava / A. R. Shendyeamol31179100% (1)
- Adobe Scan Apr 10, 2023Документ1 страницаAdobe Scan Apr 10, 2023naseemОценок пока нет
- Sensitive Posts IdentificationДокумент4 страницыSensitive Posts Identificationvital polityОценок пока нет
- Penal Demureage W e F 03 08 23Документ3 страницыPenal Demureage W e F 03 08 23Vikrant BeraОценок пока нет
- SGLGДокумент3 страницыSGLGNatacia100% (1)
- Format GPON Material - PNT - 2022-23 RUDДокумент1 страницаFormat GPON Material - PNT - 2022-23 RUDTamnna RohilaОценок пока нет
- 4th QRTR 2023Документ20 страниц4th QRTR 20232ry4mnp9rnОценок пока нет
- GIP-Badging Request 22-11-2022Документ3 страницыGIP-Badging Request 22-11-2022David RamadhanОценок пока нет
- Change in Timings of 07284 NDL-RU DEMU at RJPДокумент1 страницаChange in Timings of 07284 NDL-RU DEMU at RJPmanohar.durga93Оценок пока нет
- IRPSM NotingДокумент4 страницыIRPSM NotingNagi Reddy ChintakuntaОценок пока нет
- MSOP 2018 VariationДокумент3 страницыMSOP 2018 VariationDeepak AhujaОценок пока нет
- Merged Rate References For Areial Earth Wire QuotationДокумент29 страницMerged Rate References For Areial Earth Wire QuotationNagi Reddy ChintakuntaОценок пока нет
- Application For Registration of Dealers and Retailer/Re-Sellers of OdsДокумент2 страницыApplication For Registration of Dealers and Retailer/Re-Sellers of OdsKaren Feyt MallariОценок пока нет
- 8 Material Inspection ReportДокумент1 страница8 Material Inspection Reportvinson bayОценок пока нет
- RSA - TRG - As On 03.02.2020 - Separated - Interactive - SessionДокумент9 страницRSA - TRG - As On 03.02.2020 - Separated - Interactive - SessionTRAFFIC HRSОценок пока нет
- Sparsh 05Документ1 страницаSparsh 05Kinkar RoyОценок пока нет
- Disclosure DocumentДокумент171 страницаDisclosure DocumentManny SandichoОценок пока нет
- 67626-57 Cutoff 2 8 2023Документ1 страница67626-57 Cutoff 2 8 2023Piyush JangraОценок пока нет
- SMR RTC 2ND Quarter 2023Документ20 страницSMR RTC 2ND Quarter 20232ry4mnp9rnОценок пока нет
- JPO 19.02.2022 Rev6Документ4 страницыJPO 19.02.2022 Rev6Ajay SinghОценок пока нет
- Certificacion ISCC 2023 BiotradeДокумент2 страницыCertificacion ISCC 2023 BiotradeYMC funciones integralesОценок пока нет
- Status of Cases - RVNLДокумент1 страницаStatus of Cases - RVNLshamim ahmadОценок пока нет
- APSC Recruitment 2023Документ7 страницAPSC Recruitment 2023Nitish RaiОценок пока нет
- Revised Establishment Report Form v3 1Документ5 страницRevised Establishment Report Form v3 1Sai GuyoОценок пока нет
- MSOP Part A Item 9 (A) PDFДокумент2 страницыMSOP Part A Item 9 (A) PDFHARESH JANIОценок пока нет
- IMIRДокумент10 страницIMIRvizagnucalcuttaОценок пока нет
- GNT Dmho 08082022Документ7 страницGNT Dmho 08082022harish sappaОценок пока нет
- CBIM 2021 Form 2 - Schedule of In-Kind Local Counterpart ContributionДокумент2 страницыCBIM 2021 Form 2 - Schedule of In-Kind Local Counterpart ContributionMichael Angelo CatungalОценок пока нет
- Letter Reg. Arears of RecoveryДокумент2 страницыLetter Reg. Arears of RecoveryV.S.SharmaОценок пока нет
- Stores PT 1Документ35 страницStores PT 1Kishor Kumar VishwakarmaОценок пока нет
- Aop 2023Документ26 страницAop 2023ilog ndp100% (3)
- 1512 Comm 2023Документ9 страниц1512 Comm 2023ajaymalviya01996Оценок пока нет
- Notification SE 2017 FINALДокумент10 страницNotification SE 2017 FINALAbhisek SarangiОценок пока нет
- Establishment Employment Report RKS-Form5Документ2 страницыEstablishment Employment Report RKS-Form5Richelle WskiОценок пока нет
- Neonatology High Yield 3Документ1 страницаNeonatology High Yield 3Nirubhana ArunthavasothyОценок пока нет
- Neonatal Resuscitation - Question and AnswerДокумент3 страницыNeonatal Resuscitation - Question and AnswerNirubhana ArunthavasothyОценок пока нет
- Baby and Child First Aid 2022Документ11 страницBaby and Child First Aid 2022Nirubhana ArunthavasothyОценок пока нет
- 1 PB PDFДокумент7 страниц1 PB PDFNirubhana ArunthavasothyОценок пока нет
- MRCPCH Clinical Short Cases History Taking Communication Skills 3e PDFДокумент19 страницMRCPCH Clinical Short Cases History Taking Communication Skills 3e PDFNirubhana Arunthavasothy100% (1)
- MET Introduction at RCHДокумент3 страницыMET Introduction at RCHNirubhana ArunthavasothyОценок пока нет
- Hypoglycaemia Infant Management1Документ10 страницHypoglycaemia Infant Management1Nirubhana ArunthavasothyОценок пока нет
- Pediatric Mechanical VentilationДокумент49 страницPediatric Mechanical VentilationNirubhana ArunthavasothyОценок пока нет
- Flow, Space and Activity RelationshipsДокумент43 страницыFlow, Space and Activity RelationshipsMichael Smith86% (7)
- Principles of Management Project ReportДокумент64 страницыPrinciples of Management Project ReportAndree Chara83% (6)
- Module 6Документ47 страницModule 6Ayush GuptaОценок пока нет
- BROADBANDINGДокумент12 страницBROADBANDINGChow ChowluОценок пока нет
- NBA Draft Eligibility PaperДокумент7 страницNBA Draft Eligibility PaperMartin DunhamОценок пока нет
- Dismissal From Civil ServiceДокумент12 страницDismissal From Civil ServiceAndy MolinaОценок пока нет
- 10 Motivational TheoriesДокумент26 страниц10 Motivational TheoriessrcherОценок пока нет
- Senior Administrative Assistant ResumeДокумент6 страницSenior Administrative Assistant Resumeafjwdprlzaxewj100% (2)
- Apply 5S ProcedureДокумент18 страницApply 5S ProcedureNigussie Berhanu100% (9)
- The Gender Division of Labour. GLOPPДокумент1 страницаThe Gender Division of Labour. GLOPPMayank ShuklaОценок пока нет
- Holiday Shipping WarsДокумент8 страницHoliday Shipping WarsRajat RameshОценок пока нет
- A Literature Review of Chapter 2Документ31 страницаA Literature Review of Chapter 2dhelmharvs83% (6)
- HandbookpensionarybenefitsPBOR Oct11Документ258 страницHandbookpensionarybenefitsPBOR Oct11ama2amalОценок пока нет
- Ashok Leyland Limited: AddressДокумент2 страницыAshok Leyland Limited: AddressERAnkitMalviОценок пока нет
- PlantДокумент12 страницPlantritika5656Оценок пока нет
- DredgingДокумент57 страницDredgingHilur Muhammed100% (1)
- Public Agenda 3-5-12Документ19 страницPublic Agenda 3-5-12daniel_goodman7884Оценок пока нет
- 2011 NLRC Rules of ProcedureДокумент23 страницы2011 NLRC Rules of ProcedureDwight Aldwin GeronimoОценок пока нет
- MCQ SYBCOM 231 Business-CommunicationДокумент40 страницMCQ SYBCOM 231 Business-Communicationmitranjalee sandha0% (1)
- 2013 Kaelo BrochureДокумент3 страницы2013 Kaelo Brochureinfo7160Оценок пока нет
- Review of Related LiteratureДокумент3 страницыReview of Related LiteratureMary Grace RoqueroОценок пока нет
- Module 1Документ30 страницModule 1aagrawal3Оценок пока нет
- Effects of The Industrial RevolutionДокумент8 страницEffects of The Industrial RevolutionShabnam BarshaОценок пока нет
- Khushboo KumariДокумент60 страницKhushboo KumariDhiraj Ranjan RayОценок пока нет
- Candidate Interview Application FormДокумент1 страницаCandidate Interview Application FormAlok TiwariОценок пока нет
- IC Largest Timesheet Collection Monthly Timesheet TemplateДокумент4 страницыIC Largest Timesheet Collection Monthly Timesheet TemplateShwetha EashОценок пока нет
- Search and Unemployment: Advanced Macroeconomics Seminar 10Документ5 страницSearch and Unemployment: Advanced Macroeconomics Seminar 10vijay kumarmodiОценок пока нет