Вам также может понравиться
- EpidemiologyДокумент58 страницEpidemiologyrebecca100% (4)
- Leukemia Lesson PlanДокумент3 страницыLeukemia Lesson PlanIshika Roy75% (4)
- Leukemia Lesson PlanДокумент3 страницыLeukemia Lesson PlanIshika Roy75% (4)
- 1 - EpidemiologyДокумент26 страниц1 - Epidemiologyhemihema75% (4)
- Veterinary Epidemiology (VEP-411)Документ15 страницVeterinary Epidemiology (VEP-411)Vijay Kumar Anumolu100% (1)
- Epidemiology: Subject-Community Health NursingДокумент30 страницEpidemiology: Subject-Community Health NursingBabita Dhruw100% (3)
- Application of Orems Theory To NSG PracticeДокумент26 страницApplication of Orems Theory To NSG PracticeLorde Sungcad Ricafrente100% (3)
- Health Care Delivery System in IndiaДокумент70 страницHealth Care Delivery System in Indiaritikaritika88% (8)
- Cleaning and Disinfection Protocol For Infant IncubatorДокумент4 страницыCleaning and Disinfection Protocol For Infant Incubatorver_at_work100% (1)
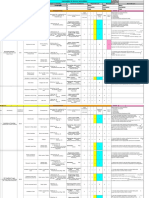
- HIRARCДокумент34 страницыHIRARCLeal Safety100% (3)
- EpidemiologyДокумент100 страницEpidemiologyKailash NagarОценок пока нет
- Epidemiology Lesson PlanДокумент7 страницEpidemiology Lesson PlanIshika RoyОценок пока нет
- Epidemiology FinalДокумент90 страницEpidemiology FinalMoumita hazarika100% (1)
- Epidemiology: RD THДокумент21 страницаEpidemiology: RD THKailash Nagar100% (1)
- Objectives of EpidemiologyДокумент23 страницыObjectives of EpidemiologyAnitha sujith75% (4)
- Basic Measures of EpidemiologyДокумент51 страницаBasic Measures of EpidemiologyHafiz SabghatullahОценок пока нет
- Epidemiology NotesДокумент16 страницEpidemiology NotesAnonymous 1I0JCC96G2100% (1)
- Seminar On Concept, Trends, Problems, and IssuesДокумент22 страницыSeminar On Concept, Trends, Problems, and IssuesAKHILA PKОценок пока нет
- EpidemiologyДокумент26 страницEpidemiologymskotОценок пока нет
- Basic Concepts of EpidemiologyДокумент125 страницBasic Concepts of EpidemiologyKailash Nagar100% (1)
- Epidemiology - IgnouДокумент25 страницEpidemiology - IgnouSujatha J JayabalОценок пока нет
- Viva-Questions Community MedicineДокумент3 страницыViva-Questions Community Medicineadeel_khan_48Оценок пока нет
- Uses of EpidemiologyДокумент18 страницUses of Epidemiologyshipra arora75% (4)
- Determinants of HealthДокумент29 страницDeterminants of HealthMayom Mabuong92% (12)
- Study To Assess The Effectiveness of Structured Teaching Programme Regarding Knowledge On Geriatric Care Among The Gerontological Nurses Working in Selected Old Age Homes in Kanyakumari DistrictДокумент10 страницStudy To Assess The Effectiveness of Structured Teaching Programme Regarding Knowledge On Geriatric Care Among The Gerontological Nurses Working in Selected Old Age Homes in Kanyakumari DistrictAntony Rose AbyОценок пока нет
- ScoringДокумент53 страницыScoringKaran SinghОценок пока нет
- Epidemiological ApproachДокумент30 страницEpidemiological ApproachRabiu Hassan Musa75% (4)
- Screening For DiseaseДокумент29 страницScreening For DiseaseSrinidhi Nandhini Pandian100% (2)
- EpidemiologyДокумент23 страницыEpidemiologyBabita DhruwОценок пока нет
- Epidemiology AssignmentДокумент12 страницEpidemiology AssignmentSagar ParajuliОценок пока нет
- National Health PolicyДокумент73 страницыNational Health PolicyHetal ChavdaОценок пока нет
- Current Trends in Community NursingДокумент9 страницCurrent Trends in Community Nursingnavasree nimmiОценок пока нет
- Sister Nivedita Government Nursing College, Igmc Shimla: Submitted To Submitted byДокумент6 страницSister Nivedita Government Nursing College, Igmc Shimla: Submitted To Submitted byshivaniОценок пока нет
- Seminar Health Care DeliveryДокумент39 страницSeminar Health Care DeliveryangayarkanniОценок пока нет
- npcdcs-22 04 2020Документ38 страницnpcdcs-22 04 2020Neethu VincentОценок пока нет
- Basic Concepts of EpidemiologyДокумент125 страницBasic Concepts of EpidemiologyKailash Nagar100% (7)
- Measures of Health PromotionДокумент68 страницMeasures of Health PromotionSamjhana Neupane100% (1)
- Level of PreventionДокумент54 страницыLevel of PreventionArun kumar100% (1)
- Intersectoral Coordination in India For Health Care AdvancementДокумент26 страницIntersectoral Coordination in India For Health Care Advancementshijoantony100% (1)
- Global Burden of DiseaseДокумент82 страницыGlobal Burden of Diseaseangayarkanni100% (1)
- StakeholderДокумент57 страницStakeholderpandem soniyaОценок пока нет
- 05 N001 40088Документ23 страницы05 N001 40088hariharad sourabhОценок пока нет
- Global Burden of DiseaseДокумент49 страницGlobal Burden of Diseasesasmita nayakОценок пока нет
- Levels of Health CareДокумент13 страницLevels of Health CareWilsonSaintsОценок пока нет
- UNIT-II-PHC AND CHC-AnandДокумент33 страницыUNIT-II-PHC AND CHC-AnandAnand gowdaОценок пока нет
- Health Information SystemДокумент11 страницHealth Information SystemVineeta Jose100% (1)
- Introductiontoepidemiology 190213062350Документ45 страницIntroductiontoepidemiology 190213062350Mangala bote Nair PSMОценок пока нет
- National Vector Borne Disease Control Programme (NVBDCP) : Presented By, Javed Khan Roll No:32Документ21 страницаNational Vector Borne Disease Control Programme (NVBDCP) : Presented By, Javed Khan Roll No:32fathima AlfasОценок пока нет
- Models of PreventionДокумент13 страницModels of Preventionsagi mu100% (1)
- Determinants of Health by VeereshДокумент12 страницDeterminants of Health by VeereshVeeresh TopalakattiОценок пока нет
- Epidemiology and The NurseДокумент26 страницEpidemiology and The NurseCris Melric Palanog100% (3)
- MSC Disseration ProjectsДокумент12 страницMSC Disseration ProjectsKowsalyaram RamОценок пока нет
- Information Communication EducationДокумент19 страницInformation Communication EducationNarjina Begam100% (1)
- ApproachesДокумент22 страницыApproacheskles insgkk100% (1)
- Public Private Partnership: By: Ms. Priyanka Bansal Msc. Nursing-I Year Rufaida College of NursingДокумент28 страницPublic Private Partnership: By: Ms. Priyanka Bansal Msc. Nursing-I Year Rufaida College of NursingPriyanka BansalОценок пока нет
- FY MSC Community Health Nursing Clinical Specialty IДокумент4 страницыFY MSC Community Health Nursing Clinical Specialty IPriya Sharma100% (1)
- Ors, Hyd Mix& Road To H CardДокумент10 страницOrs, Hyd Mix& Road To H CardAnonymous hYMWbAОценок пока нет
- List of Important Health Days: World Consumer Rights DayДокумент0 страницList of Important Health Days: World Consumer Rights DayAnnapurna DangetiОценок пока нет
- Health Care Delivery System in IndiaДокумент11 страницHealth Care Delivery System in IndiaAnish VeettiyankalОценок пока нет
- Management of Tuberculosis: A guide for clinicians (eBook edition)От EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)Оценок пока нет
- Chapter 101 EpidemiologyДокумент44 страницыChapter 101 EpidemiologyYassir OunsaОценок пока нет
- Science of Epidemiology-31.8.'16 Modified On 23.10.2016Документ7 страницScience of Epidemiology-31.8.'16 Modified On 23.10.2016Alankrit PatnaikОценок пока нет
- Lecturenote - 2121234844biostatistics and Epidemiology (Stat3101) Handout Chapter-1Документ20 страницLecturenote - 2121234844biostatistics and Epidemiology (Stat3101) Handout Chapter-1McLord SelasiОценок пока нет
- Case Presentation IOДокумент14 страницCase Presentation IOIshika RoyОценок пока нет
- Draft of CARE OF A CHILD IN VENTILATORДокумент52 страницыDraft of CARE OF A CHILD IN VENTILATORIshika Roy100% (1)
- Care of Newborn With Long Term Ventilator PDFДокумент6 страницCare of Newborn With Long Term Ventilator PDFIshika Roy100% (1)
- Pediatric Assessment SheetДокумент6 страницPediatric Assessment SheetIshika RoyОценок пока нет
- B.SC Nursing 1Документ2 страницыB.SC Nursing 1Ishika RoyОценок пока нет
- SignatureДокумент2 страницыSignatureIshika RoyОценок пока нет
- Care of Newborn With Long Term Ventilator PDFДокумент6 страницCare of Newborn With Long Term Ventilator PDFIshika Roy100% (1)
- Textbook of Microbiology by Baveja PDFДокумент3 страницыTextbook of Microbiology by Baveja PDFIshika Roy0% (2)
- Bibliography PedДокумент1 страницаBibliography PedIshika RoyОценок пока нет
- Lesson Plan Format FinalДокумент6 страницLesson Plan Format FinalIshika RoyОценок пока нет
- SignatureДокумент2 страницыSignatureIshika RoyОценок пока нет
- B.SC Nursing 1Документ2 страницыB.SC Nursing 1Ishika RoyОценок пока нет
- ICFAI Business SchoolДокумент3 страницыICFAI Business SchoolIshika Roy100% (1)
- Nursing Education Field TripДокумент5 страницNursing Education Field TripIshika Roy67% (3)
- M.sc. Nursing Syllabus 0108Документ142 страницыM.sc. Nursing Syllabus 0108Nikhil DahiyaОценок пока нет
- Antenatal CareДокумент19 страницAntenatal CareIshika RoyОценок пока нет
- Seminar ON Imnci: (Integrated Management of Neonatal and Childhood Illness)Документ1 страницаSeminar ON Imnci: (Integrated Management of Neonatal and Childhood Illness)Ishika RoyОценок пока нет
- Nursing Education Field TripДокумент5 страницNursing Education Field TripIshika Roy67% (3)
- EpidemiologyДокумент32 страницыEpidemiologyIshika RoyОценок пока нет
- High Risk Scoring 1Документ4 страницыHigh Risk Scoring 1Ishika RoyОценок пока нет
- Content ON Measurement in Epidemiology Mortality and MorbidityДокумент13 страницContent ON Measurement in Epidemiology Mortality and MorbidityIshika Roy100% (1)
- 2Документ8 страниц2Ishika RoyОценок пока нет
- 2Документ4 страницы2Ishika RoyОценок пока нет
- Curriculum Vitaé: Work-ExperienceДокумент2 страницыCurriculum Vitaé: Work-ExperienceIshika RoyОценок пока нет
- Project - Tapan KR MandalДокумент9 страницProject - Tapan KR MandalIshika RoyОценок пока нет
- Steps in Undertaking Preliminary Investigation: 1.) Screening TestsДокумент2 страницыSteps in Undertaking Preliminary Investigation: 1.) Screening TestsApril Rose SalvadicoОценок пока нет
- Interpretation of Hepatitis B Serologic Test ResultsДокумент1 страницаInterpretation of Hepatitis B Serologic Test ResultsMUHAMMAD JAWAD HASSANОценок пока нет
- Dengue Thesis Final Giebacolod.Документ91 страницаDengue Thesis Final Giebacolod.Leo Sindol33% (3)
- Health and Wellness Women HealthДокумент24 страницыHealth and Wellness Women HealthShimmering MoonОценок пока нет
- Lesson PlanДокумент5 страницLesson PlanDranlie LagdamenОценок пока нет
- Plot No.7G, Ground Floor, Opp. Graphite India, Telerad RXDX Healthcare PVT LTDДокумент4 страницыPlot No.7G, Ground Floor, Opp. Graphite India, Telerad RXDX Healthcare PVT LTDSanjay TripathiОценок пока нет
- Acute Infections During PregnancyДокумент63 страницыAcute Infections During PregnancyHussein AliОценок пока нет
- Hyperemesis GravidarumДокумент6 страницHyperemesis GravidarumKeii blackhoodОценок пока нет
- Prevalence and Impact of Diabetes Among People Infected With Sars Cov 2Документ3 страницыPrevalence and Impact of Diabetes Among People Infected With Sars Cov 2Maulana AkbarОценок пока нет
- National Rural Health Alliance: Nicki Welch, February 2000Документ13 страницNational Rural Health Alliance: Nicki Welch, February 2000Chia Xin LooОценок пока нет
- UNICEF Nutrition Strategy 2020-2030Документ110 страницUNICEF Nutrition Strategy 2020-2030jacob100% (1)
- Mutiple - Reading ComprehensionДокумент8 страницMutiple - Reading ComprehensionVan AnhОценок пока нет
- Allergic Reaction Typhoid Vaccine: Side Effects Associated With Typhoid Fever VaccinesДокумент2 страницыAllergic Reaction Typhoid Vaccine: Side Effects Associated With Typhoid Fever VaccinesAnis AmaninaОценок пока нет
- Previous Year 6th SemesterДокумент58 страницPrevious Year 6th SemesterYash Raj GairaОценок пока нет
- Stunting, Women's Nutrition and South Asia: Dr. Sheila C VirДокумент40 страницStunting, Women's Nutrition and South Asia: Dr. Sheila C VirMuchrizal CorpОценок пока нет
- Effectiveness of Finger Held Relaxation On The Decrease in Intensity of Pain in Patient of Post-Sectio Caesarea in RSUD Sorong RegencyДокумент4 страницыEffectiveness of Finger Held Relaxation On The Decrease in Intensity of Pain in Patient of Post-Sectio Caesarea in RSUD Sorong RegencyFebita BellaОценок пока нет
- Vaxigrip Tetra Pi Nh19-20Документ2 страницыVaxigrip Tetra Pi Nh19-20A. shahizaОценок пока нет
- Communicable DiseasesДокумент18 страницCommunicable DiseasesLeoAtienzaОценок пока нет
- D.Pharm 1 Year ER20-15T-Social Pharmacy: TuberculosisДокумент33 страницыD.Pharm 1 Year ER20-15T-Social Pharmacy: TuberculosisPriyanshu SharmaОценок пока нет
- Philippines in The Midst of The Pandemic: TH NDДокумент2 страницыPhilippines in The Midst of The Pandemic: TH NDLance DagdagОценок пока нет
- MCN Doc PacabisДокумент18 страницMCN Doc PacabisSJane FeriaОценок пока нет
- Test-I. Multiple Choice. Choose The Correct Answer From The Choices Given. Write Only The Letter On TheДокумент5 страницTest-I. Multiple Choice. Choose The Correct Answer From The Choices Given. Write Only The Letter On TheJobert eulatrizОценок пока нет
- Hand Hygiene and HandwashingДокумент7 страницHand Hygiene and HandwashingFaith Dianasas RequinaОценок пока нет
- CPG PerinatalДокумент7 страницCPG PerinatalReuter Lloyd MarianoОценок пока нет
- Oec-Covid-19-Guidance-For-Child-Care June 1Документ25 страницOec-Covid-19-Guidance-For-Child-Care June 1api-244363080Оценок пока нет
- Healthcare System in RomaniaДокумент14 страницHealthcare System in RomaniaanitudoseОценок пока нет
- Policy - Partners or Support People Staying Overnight at Wellington HospitalДокумент3 страницыPolicy - Partners or Support People Staying Overnight at Wellington HospitalStuff NewsroomОценок пока нет
- Cesarean Section Audit FormatДокумент6 страницCesarean Section Audit FormatRahul JalauniaОценок пока нет