Вам также может понравиться
- CM All Compiled NotesДокумент100 страницCM All Compiled NotesKatrina Mae PatalinghugОценок пока нет
- Clinical Microscopy: Definition and Volume Disease and Cause PolyuriaДокумент5 страницClinical Microscopy: Definition and Volume Disease and Cause PolyuriaJovanni andesОценок пока нет
- Clinical MicrosДокумент26 страницClinical MicrosDarla YsavelОценок пока нет
- Clinical Microscopy: Capture All The POO/PEE!!!Документ54 страницыClinical Microscopy: Capture All The POO/PEE!!!VenomОценок пока нет
- Intro To Urinalysis TransДокумент5 страницIntro To Urinalysis Transapril jholynna garroОценок пока нет
- Reanalyze PDFДокумент32 страницыReanalyze PDFpikachuОценок пока нет
- CM Handouts Clinical MicrosДокумент33 страницыCM Handouts Clinical Microsrenato renato100% (1)
- Aubf Lec M1-M2Документ8 страницAubf Lec M1-M2Erica Rance TambaОценок пока нет
- Examination of Body FluidsДокумент14 страницExamination of Body Fluidskiedd_04100% (11)
- By: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Документ61 страницаBy: Dr. Yoavita Moderator: Dr. Anik Widijanti, SP - PK (K)Gilang KusdinarОценок пока нет
- UrinalysisДокумент172 страницыUrinalysisRonelene GatoОценок пока нет
- Biochemistry Laboratory Manual Group 2: 2. Enumerate The Different Methods of Preserving A Urine SampleДокумент18 страницBiochemistry Laboratory Manual Group 2: 2. Enumerate The Different Methods of Preserving A Urine SampleMonique BorresОценок пока нет
- Urine Physical Sediment1819Документ23 страницыUrine Physical Sediment1819Anas ShwbkОценок пока нет
- UrinalysisДокумент67 страницUrinalysisumairzafar5261Оценок пока нет
- Urine JSJ EoДокумент9 страницUrine JSJ EokeiОценок пока нет
- Analysis of Abnormal UrineДокумент12 страницAnalysis of Abnormal Urinesingonstrings365Оценок пока нет
- 1st Week Aubf Mtap and Semr FinalsДокумент48 страниц1st Week Aubf Mtap and Semr FinalsKrenz CatiboОценок пока нет
- Chapter 2 Introduction To Urinalysis PDFДокумент4 страницыChapter 2 Introduction To Urinalysis PDFJulie Anne Soro ValdezОценок пока нет
- Clinical MicrosДокумент14 страницClinical MicrosKRISTINE JOY PANGAHINОценок пока нет
- MLSP MidtermДокумент14 страницMLSP MidtermANGELICA ROMAWAKОценок пока нет
- Routine FecalysisДокумент25 страницRoutine FecalysisE. B. F.Оценок пока нет
- Urine Analysis FinalДокумент112 страницUrine Analysis FinalNischita JayarajОценок пока нет
- Clinical Microscopy (Analysis of Urine and Other Body Fluids)Документ14 страницClinical Microscopy (Analysis of Urine and Other Body Fluids)Jeanly DoctorОценок пока нет
- Ex1 - Specimen CollectionДокумент6 страницEx1 - Specimen CollectionRedelle Mae NiniОценок пока нет
- AUBF - Chapter 2Документ5 страницAUBF - Chapter 2Kristin SoquilloОценок пока нет
- 1.6.5.4c - URINALISISДокумент30 страниц1.6.5.4c - URINALISISBilqis ElfariantiОценок пока нет
- Analysis of UrineДокумент22 страницыAnalysis of UrineFaith Domingo100% (1)
- Rine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al MaqadmaДокумент39 страницRine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al Maqadmaiman zainuddinОценок пока нет
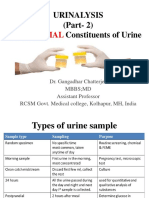
- Urinalysis (Part-2) Constituents of Urine: AbnormalДокумент49 страницUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshОценок пока нет
- AUBF Lesson UrinalysisДокумент5 страницAUBF Lesson UrinalysisReyn CrisostomoОценок пока нет
- AUBF Laboratory Exercise I-AДокумент6 страницAUBF Laboratory Exercise I-AVelez LecturesОценок пока нет
- Bayombong, Nueva Vizcaya 3700 Nursing DepartmentДокумент7 страницBayombong, Nueva Vizcaya 3700 Nursing DepartmentKyla CarbonelОценок пока нет
- UrinalysisДокумент35 страницUrinalysisAbdulelah MurshidОценок пока нет
- Abnormal UrineДокумент28 страницAbnormal UrinemujeebОценок пока нет
- Experiment 5 Urine AnalysisДокумент7 страницExperiment 5 Urine AnalysisKenth Roger A. MaquilingОценок пока нет
- 2.1 Physical Examination 033230Документ24 страницы2.1 Physical Examination 033230Taladua Cayla Grace O.Оценок пока нет
- UrinalysisДокумент10 страницUrinalysisMichelle100% (2)
- Stool Analysis: What Is The Stool or Feces?Документ28 страницStool Analysis: What Is The Stool or Feces?Annisa SafiraОценок пока нет
- Aubf LecДокумент66 страницAubf Lec12 Newton - Cayetano, Arafe Nicole A.Оценок пока нет
- 4 Urineanalysis 121116102335 Phpapp01Документ32 страницы4 Urineanalysis 121116102335 Phpapp01bnmjgcОценок пока нет
- Urine AnalysisДокумент32 страницыUrine AnalysisbnmjgcОценок пока нет
- Chemical Examination of UrineДокумент18 страницChemical Examination of UrineYasmeen JovesОценок пока нет
- Examination of Body Fluids (Urinalysis)Документ109 страницExamination of Body Fluids (Urinalysis)kiedd_04100% (9)
- Urease Test - Principle, Media, Procedure and ResultДокумент11 страницUrease Test - Principle, Media, Procedure and ResultAlisha KhanОценок пока нет
- 1 - Introduction To UrinalysisДокумент6 страниц1 - Introduction To UrinalysisKunware TropaОценок пока нет
- StoolДокумент28 страницStoolThampron ThongphanОценок пока нет
- UrinalysisДокумент83 страницыUrinalysisJasneetaОценок пока нет
- URINALYSISДокумент80 страницURINALYSISredr7131Оценок пока нет
- Urine-Analysis 140420Документ74 страницыUrine-Analysis 140420sabao kizuiteОценок пока нет
- Choler A: Prepared By: Angelou Mortos John Radley SantosДокумент11 страницCholer A: Prepared By: Angelou Mortos John Radley SantosAdhaОценок пока нет
- CHARACTERISTICS OF SEWAGE: Analysis RequiredДокумент7 страницCHARACTERISTICS OF SEWAGE: Analysis RequiredJade Paul D. BesanaОценок пока нет
- 2.physical ch. urine د.هناديДокумент22 страницы2.physical ch. urine د.هناديAbdulmalik Al-harthyОценок пока нет
- Lab Report 1 UrinalysisДокумент7 страницLab Report 1 UrinalysisAtiqah Yeo86% (21)
- MetabolismДокумент58 страницMetabolismZ ZernsОценок пока нет
- Abnormal Constituents of Urine Interpretation PracticalДокумент42 страницыAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiОценок пока нет
- Urine ExaminationДокумент8 страницUrine ExaminationAnban SureshОценок пока нет
- Chemical Examination of UrineДокумент46 страницChemical Examination of UrineH GondaliyaОценок пока нет
- The Large IntestineДокумент33 страницыThe Large IntestineElena ParadiseОценок пока нет
- DR - Layla Abd Alasattar Sadiq Laylani: PHD PhysiologyДокумент13 страницDR - Layla Abd Alasattar Sadiq Laylani: PHD PhysiologyAkAm 33 ꪜОценок пока нет
- Acidosis: Clinical Aspects and Treatment with Isotonic Sodium Bicarbonate SolutionОт EverandAcidosis: Clinical Aspects and Treatment with Isotonic Sodium Bicarbonate SolutionРейтинг: 5 из 5 звезд5/5 (1)
- Danao John Glenn V. Corporation LawДокумент1 страницаDanao John Glenn V. Corporation LawGlennОценок пока нет
- TAX 01 General PrinciplesДокумент5 страницTAX 01 General PrinciplesGlennОценок пока нет
- Philippines 1987 PDFДокумент67 страницPhilippines 1987 PDFGlennОценок пока нет
- Kuisioner Self CareДокумент3 страницыKuisioner Self CareLeni Pertiwi PutriОценок пока нет
- The National Teachers CollegeДокумент1 страницаThe National Teachers CollegeGlennОценок пока нет
- Endocrinology - Polyuria - SOAP Note - Jeanette GoguenДокумент3 страницыEndocrinology - Polyuria - SOAP Note - Jeanette GoguenFrancieudo SampaioОценок пока нет
- Ii. Hydroelectrolytic Imbalance PDFДокумент30 страницIi. Hydroelectrolytic Imbalance PDFIvanes IgorОценок пока нет
- Fluid & Electrolyte Quiz 1Документ2 страницыFluid & Electrolyte Quiz 1Marti Gregorio100% (1)
- Posterior Pituitary: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeДокумент60 страницPosterior Pituitary: DR Axelle Saverettiar Mbbs Physiology Department SSR Medical CollegeÑäd ÉèmОценок пока нет
- Siadh and Di QuestionsДокумент18 страницSiadh and Di QuestionsRegiever Salvante100% (1)
- ICU ReadingДокумент24 страницыICU Reading駱品全Оценок пока нет
- Diabetes InsipidusДокумент48 страницDiabetes InsipidusAhmed Fraz MamoonОценок пока нет
- Polydipsia & Polyuria Tutorial, March 16,3Документ45 страницPolydipsia & Polyuria Tutorial, March 16,3Abdurazzag ShumakhiОценок пока нет
- SIADH, DI and Cerebral Salt Wasting: Karim Rafaat, MDДокумент54 страницыSIADH, DI and Cerebral Salt Wasting: Karim Rafaat, MDMahendra PrasetyoОценок пока нет
- Diabetes Insipidus: CausesДокумент3 страницыDiabetes Insipidus: CausesjudssalangsangОценок пока нет
- NCLEX Practice Test For Endocrine Disorders Part 2Документ16 страницNCLEX Practice Test For Endocrine Disorders Part 2Hasan A AsFourОценок пока нет
- Disorders Due To Hormone Deficiency (Hyposecretion) : List of Hormonal DisordersДокумент2 страницыDisorders Due To Hormone Deficiency (Hyposecretion) : List of Hormonal Disordersritik shuklaОценок пока нет
- NCM 116 Midterm PDFДокумент130 страницNCM 116 Midterm PDFPonciana PasanaОценок пока нет
- Anesthesia For Transsphenoidal Pituitary Surgery.Документ6 страницAnesthesia For Transsphenoidal Pituitary Surgery.ismaelОценок пока нет
- AUB - Physical Examination of UrineДокумент3 страницыAUB - Physical Examination of UrineJeanne RodiñoОценок пока нет
- 55 ENDOCRINE Tutorial Week 5AДокумент9 страниц55 ENDOCRINE Tutorial Week 5AChristian Versola-Macapulay Valle100% (1)
- Body Fluid CompartmentsДокумент37 страницBody Fluid Compartmentsmanu sethiОценок пока нет
- Mtap421 ElectrolytesДокумент9 страницMtap421 ElectrolytesNhelomar ManlinconОценок пока нет
- Introduction To UrinalysisДокумент28 страницIntroduction To UrinalysisNicnoc RiveraОценок пока нет
- Canine and Feline Endocrinology and ReproductionДокумент1 095 страницCanine and Feline Endocrinology and ReproductionmarparolaОценок пока нет
- Med SurgДокумент23 страницыMed SurgReymart AcalaОценок пока нет
- Hypernatremia in Children - UpToDateДокумент25 страницHypernatremia in Children - UpToDateDiego Chimbo NicolaldeОценок пока нет
- Endocrinology 2Документ108 страницEndocrinology 2moad kiОценок пока нет
- Ilovepathology - Com (1) UrinДокумент2 страницыIlovepathology - Com (1) UrinNori VeilaОценок пока нет
- Diabetes Insipidus (Definition and Clinical Manifestation)Документ2 страницыDiabetes Insipidus (Definition and Clinical Manifestation)Norbert Ju NeОценок пока нет
- Endocrine Disorders (Study Notes)Документ11 страницEndocrine Disorders (Study Notes)Danelle Harrison, RN90% (10)
- Endocrine System - LectureДокумент213 страницEndocrine System - LectureRosita Antiquina Elopre100% (1)
- Endocrine DisorderДокумент5 страницEndocrine DisorderMenly SusadaОценок пока нет
- Diabetes Causes and SympthomsДокумент24 страницыDiabetes Causes and SympthomsTinke WinkeОценок пока нет
- MRCPass Notes For MRCP 1 - EnDOCRINOLOGYДокумент12 страницMRCPass Notes For MRCP 1 - EnDOCRINOLOGYsabdali100% (1)