Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Kyasanur Forest Disease, India, 2011-2012Документ4 страницыKyasanur Forest Disease, India, 2011-2012Zona Educación Especial ZacapaoaxtlaОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- MqoДокумент30 страницMqoZona Educación Especial ZacapaoaxtlaОценок пока нет
- Seajphv 3 N 1 P 8Документ14 страницSeajphv 3 N 1 P 8Zona Educación Especial ZacapaoaxtlaОценок пока нет
- 3-Band Preamp & Direct Box Owner's GuideДокумент2 страницы3-Band Preamp & Direct Box Owner's GuideZona Educación Especial ZacapaoaxtlaОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- MqiДокумент22 страницыMqiZona Educación Especial ZacapaoaxtlaОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The World of ZKW 2018Документ23 страницыThe World of ZKW 2018Zona Educación Especial ZacapaoaxtlaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- 3-Band Preamp & Direct Box Owner's GuideДокумент2 страницы3-Band Preamp & Direct Box Owner's GuideZona Educación Especial ZacapaoaxtlaОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Investigation of The Influence of Vanadium Compounds Treatment in Nzo Mice Model Ñ Preliminary StudyДокумент8 страницInvestigation of The Influence of Vanadium Compounds Treatment in Nzo Mice Model Ñ Preliminary StudyZona Educación Especial ZacapaoaxtlaОценок пока нет
- Note Guidance Maximum Shelf Life Sterile Products Human Use After First Opening Following enДокумент2 страницыNote Guidance Maximum Shelf Life Sterile Products Human Use After First Opening Following enZona Educación Especial ZacapaoaxtlaОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Datenblatt Traxon DotXLQ 8 RGBW 201706AДокумент5 страницDatenblatt Traxon DotXLQ 8 RGBW 201706AZona Educación Especial ZacapaoaxtlaОценок пока нет
- Quick Guide to Getting Started with MoqДокумент12 страницQuick Guide to Getting Started with MoqZona Educación Especial ZacapaoaxtlaОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Engine Cooling System: SectionДокумент60 страницEngine Cooling System: SectionZona Educación Especial ZacapaoaxtlaОценок пока нет
- IJP Volume 5 Issue 7 Pages 5391-5400Документ10 страницIJP Volume 5 Issue 7 Pages 5391-5400Zona Educación Especial ZacapaoaxtlaОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Spring 2014Документ32 страницыSpring 2014Zona Educación Especial ZacapaoaxtlaОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- History of East Asian Martial ArtsДокумент7 страницHistory of East Asian Martial ArtsZona Educación Especial ZacapaoaxtlaОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Efficient profile measurement with the KHT ProfileScanДокумент4 страницыEfficient profile measurement with the KHT ProfileScanZona Educación Especial ZacapaoaxtlaОценок пока нет
- Miniture Glass Fuse GSB-GDGДокумент1 страницаMiniture Glass Fuse GSB-GDGZona Educación Especial ZacapaoaxtlaОценок пока нет
- LanДокумент90 страницLanZona Educación Especial ZacapaoaxtlaОценок пока нет
- Info 116 enДокумент87 страницInfo 116 enZona Educación Especial ZacapaoaxtlaОценок пока нет
- 5683Документ1 страница5683Zona Educación Especial ZacapaoaxtlaОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Cruise Control System: SectionДокумент3 страницыCruise Control System: SectionZona Educación Especial ZacapaoaxtlaОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- Charging System: SectionДокумент30 страницCharging System: SectionZona Educación Especial ZacapaoaxtlaОценок пока нет
- DLKДокумент144 страницыDLKJUAN CARLOS PAZОценок пока нет
- KHT Brochure enДокумент7 страницKHT Brochure enZona Educación Especial ZacapaoaxtlaОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- MwiДокумент91 страницаMwiZona Educación Especial ZacapaoaxtlaОценок пока нет
- RSUДокумент13 страницRSUJUAN CARLOS PAZОценок пока нет
- Ventilation, heater and air conditioner maintenance and repair guideДокумент27 страницVentilation, heater and air conditioner maintenance and repair guideZona Educación Especial ZacapaoaxtlaОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
- SEДокумент51 страницаSEZona Educación Especial ZacapaoaxtlaОценок пока нет
- RAXДокумент25 страницRAXZona Educación Especial ZacapaoaxtlaОценок пока нет
- Appointment Letter Staff Nurse Job DescriptionДокумент3 страницыAppointment Letter Staff Nurse Job DescriptionRenita ChrisОценок пока нет
- Production Chemistry and Flow Assurance SimulationДокумент21 страницаProduction Chemistry and Flow Assurance SimulationWael Badri100% (1)
- NEOM-NDS-SPC-015 - 01.00 - Neutral Earthing Resistor (NER) SpecificationДокумент15 страницNEOM-NDS-SPC-015 - 01.00 - Neutral Earthing Resistor (NER) Specificationcawoc96196Оценок пока нет
- PCOS Diet Cookbook For Newly Diagnosed IndividualsДокумент67 страницPCOS Diet Cookbook For Newly Diagnosed Individualsmavendave4lifeОценок пока нет
- ODN102001 ATN Products Hardware Introduction ISSUE 1.00Документ43 страницыODN102001 ATN Products Hardware Introduction ISSUE 1.00Jonathan Eduardo Tapias BeltranОценок пока нет
- Ic M423GДокумент2 страницыIc M423GSerikhi AliОценок пока нет
- Fosfomycin: Review and Use Criteria BackgroundДокумент12 страницFosfomycin: Review and Use Criteria BackgroundAbu Azzam Al-Hadi100% (1)
- Rotation: Medical Intensive Care Unit (South Campus) For Interns and ResidentsДокумент6 страницRotation: Medical Intensive Care Unit (South Campus) For Interns and ResidentsHashimIdreesОценок пока нет
- Septic Abortion PDFДокумент4 страницыSeptic Abortion PDFmariachrismayaniОценок пока нет
- Torc 4 Abscohort1 - CompressДокумент13 страницTorc 4 Abscohort1 - CompressFaye MartinezОценок пока нет
- Pathology AIIMSДокумент26 страницPathology AIIMSvkОценок пока нет
- Fuente As-IДокумент4 страницыFuente As-IadalaviОценок пока нет
- Sprocket Asa 180Документ1 страницаSprocket Asa 180jhampolrosalesОценок пока нет
- Separation Processes Lecture 1 IntroductionДокумент14 страницSeparation Processes Lecture 1 Introductionabood assrfndyОценок пока нет
- M&SДокумент39 страницM&Sgo.pushp70910% (1)
- 2.factory Price - Alarm Accessories-Complete 20150325Документ15 страниц2.factory Price - Alarm Accessories-Complete 20150325FREE BUSINESS INTELLIGENCEОценок пока нет
- STC Bec Wir Plu D 0209 01 PDFДокумент10 страницSTC Bec Wir Plu D 0209 01 PDFAdel MorsyОценок пока нет
- 2002 - Comparison of The Absorption of Micronized (Daflon 500 MG) and Nonmicronized 14c-Diosmin TabletsДокумент9 страниц2002 - Comparison of The Absorption of Micronized (Daflon 500 MG) and Nonmicronized 14c-Diosmin TabletsMai HuynhОценок пока нет
- RMD - Lightmix Modular CE IVD Assay BrochureДокумент4 страницыRMD - Lightmix Modular CE IVD Assay BrochureDummy Tester JrОценок пока нет
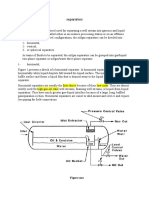
- Separators: Figure OneДокумент8 страницSeparators: Figure OneMohamed Moder100% (1)
- Folder Hexa EngДокумент8 страницFolder Hexa EngMuresan MVОценок пока нет
- E06 Power Cable Joints and Terminations v1Документ20 страницE06 Power Cable Joints and Terminations v1Anorld WalkerОценок пока нет
- Paragenesis of OlivineДокумент18 страницParagenesis of OlivineSyed Zaman100% (2)
- Schlumber: Kevin: 16010072 Moch Rizky Setiawan: 16010068Документ12 страницSchlumber: Kevin: 16010072 Moch Rizky Setiawan: 16010068KevinОценок пока нет
- DILEM 10 G (24VDC) MoellerДокумент7 страницDILEM 10 G (24VDC) MoellerElizabeth RamirezОценок пока нет
- Water For Injections BP: What Is in This Leaflet?Документ2 страницыWater For Injections BP: What Is in This Leaflet?Mohamed OmerОценок пока нет
- Compabloc Heat Exchangers Cut Downtime at Nynäs RefineryДокумент2 страницыCompabloc Heat Exchangers Cut Downtime at Nynäs RefinerylaythОценок пока нет
- Guided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Документ5 страницGuided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Chenie BatacОценок пока нет
- 01 Well Head ComponentsДокумент46 страниц01 Well Head ComponentsKhanh Pham Minh100% (7)
- Earth First! Climbers Guild Vol. 2Документ16 страницEarth First! Climbers Guild Vol. 2CascadiaDefenders100% (2)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (18)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (78)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет