Вам также может понравиться
- James W. Hardin, Joseph M. Hilbe - Generalized Linear Models and Extensions-Stata Press (2018)Документ789 страницJames W. Hardin, Joseph M. Hilbe - Generalized Linear Models and Extensions-Stata Press (2018)owusuessel100% (1)
- Academic Unit of General Practice: 2019 Newsletter - Semester 2, Christmas EditionДокумент8 страницAcademic Unit of General Practice: 2019 Newsletter - Semester 2, Christmas EditionowusuesselОценок пока нет
- Gender Inequality IndexДокумент16 страницGender Inequality IndexowusuesselОценок пока нет
- E94296 PDFДокумент54 страницыE94296 PDFowusuesselОценок пока нет
- Spatial Analysis of Skilled Birth Attendant Utilization in GhanaДокумент12 страницSpatial Analysis of Skilled Birth Attendant Utilization in GhanaowusuesselОценок пока нет
- CMSA General Guidelines Booklet - 4 May 2017 20-7-2018Документ92 страницыCMSA General Guidelines Booklet - 4 May 2017 20-7-2018owusuessel100% (1)
- Health Policy: Kristin Farrants, Clare Bambra, Lotta Nylen, Adetayo Kasim, Bo Burström, David HunterДокумент8 страницHealth Policy: Kristin Farrants, Clare Bambra, Lotta Nylen, Adetayo Kasim, Bo Burström, David HunterowusuesselОценок пока нет
- Diagnosis of Urethral Diverticulum Mimicking Pelvic Organ Prolapse With Translabial UltrasonographyДокумент1 страницаDiagnosis of Urethral Diverticulum Mimicking Pelvic Organ Prolapse With Translabial UltrasonographyowusuesselОценок пока нет
- Primary Papillary Serous Carcinoma of The Fallopian Tube Presenting As A Vaginal Mass: A Case Report and Review of The LiteratureДокумент6 страницPrimary Papillary Serous Carcinoma of The Fallopian Tube Presenting As A Vaginal Mass: A Case Report and Review of The LiteratureowusuesselОценок пока нет
- Environment International: SciencedirectДокумент8 страницEnvironment International: SciencedirectowusuesselОценок пока нет
- Cesarean Scar Pregnancy Associated With An Impending Uterine Rupture Diagnosed With 3-Dimensional UltrasonographyДокумент2 страницыCesarean Scar Pregnancy Associated With An Impending Uterine Rupture Diagnosed With 3-Dimensional UltrasonographyowusuesselОценок пока нет
- Health Policy: Sarah-Jo Sinnott, Helen Whelton, Jessica Myers Franklin, Jennifer Milan PolinskiДокумент8 страницHealth Policy: Sarah-Jo Sinnott, Helen Whelton, Jessica Myers Franklin, Jennifer Milan PolinskiowusuesselОценок пока нет
- 1 s2.0 S0002937816308225 MainДокумент1 страница1 s2.0 S0002937816308225 MainowusuesselОценок пока нет
- Critical Appraisal of The Paper TitledДокумент3 страницыCritical Appraisal of The Paper TitledowusuesselОценок пока нет
- Payment MethodsДокумент4 страницыPayment MethodsowusuesselОценок пока нет
- Wacs Accreditation StatusДокумент4 страницыWacs Accreditation StatusowusuesselОценок пока нет
- Wacp Primary Curriculum For Psychiatry PDFДокумент5 страницWacp Primary Curriculum For Psychiatry PDFowusuesselОценок пока нет
- Cervical Cancer: Presented at Bole Methodist Church, NRДокумент39 страницCervical Cancer: Presented at Bole Methodist Church, NRowusuesselОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Giovan Cosimo Bonomo (1663-1696) - Discoverer of The Etiology of ScabiesДокумент8 страницGiovan Cosimo Bonomo (1663-1696) - Discoverer of The Etiology of ScabiesPratik PatelОценок пока нет
- Insights From Veterinary MedicineДокумент290 страницInsights From Veterinary Medicinenorma paulina carcausto lipaОценок пока нет
- 2020 PBR CORRECTIONS AND CLARIFICATIONS GUIDE - 2021 ImagesДокумент80 страниц2020 PBR CORRECTIONS AND CLARIFICATIONS GUIDE - 2021 ImagespbradminОценок пока нет
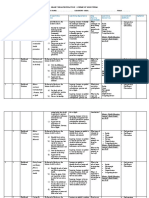
- Grade 7 SchemesДокумент7 страницGrade 7 SchemesMalesi SiemaОценок пока нет
- Scabies Questions and AnswersДокумент15 страницScabies Questions and AnswersCandra Adie Wicahyono100% (1)
- ScabiesДокумент6 страницScabiesJayson ShieldsОценок пока нет
- Original Research Article - Controlling Scabies in Madrasahs (Islamic Religious Schools) in BangladeshДокумент9 страницOriginal Research Article - Controlling Scabies in Madrasahs (Islamic Religious Schools) in BangladeshMuhammad IkbarОценок пока нет
- Common Child and AdolescentДокумент23 страницыCommon Child and AdolescentValeria BeltranОценок пока нет
- My Cat Scratched Me and A Weird Welt Formed Around It - MildlyinterestingДокумент12 страницMy Cat Scratched Me and A Weird Welt Formed Around It - MildlyinterestingGoo GleОценок пока нет
- Np1 July2021 ActualДокумент15 страницNp1 July2021 ActualAnnizaОценок пока нет
- Nclex BulletsДокумент34 страницыNclex Bulletssaroberts2202100% (1)
- Permethrin Topical Cream RLD 019855 RC08-17Документ7 страницPermethrin Topical Cream RLD 019855 RC08-17Ritesh RastogiОценок пока нет
- Akwanwa Botanics Full Skincare EbookДокумент150 страницAkwanwa Botanics Full Skincare EbookChinaemerem83% (6)
- CASE 4 PharmaДокумент2 страницыCASE 4 PharmaJoana Mikee RasayОценок пока нет
- Nursing Management of Skin and Parasitic DiseasesДокумент14 страницNursing Management of Skin and Parasitic Diseasesyer tagalajОценок пока нет
- Rash Potpourri Didacticwith AnimationДокумент75 страницRash Potpourri Didacticwith AnimationFlavius AnghelОценок пока нет
- Jurnal Scabies 7Документ9 страницJurnal Scabies 7Eric FullerОценок пока нет
- Skin ConditionsДокумент43 страницыSkin ConditionspdladvaОценок пока нет
- Scabies.: Vanessa ChelimoДокумент19 страницScabies.: Vanessa ChelimoAlvin OmondiОценок пока нет
- Integumentary Disorders (New)Документ41 страницаIntegumentary Disorders (New)coosa liquorsОценок пока нет
- Daily Lesson Plan - NSTP1Документ3 страницыDaily Lesson Plan - NSTP1Charity Mae DoradoОценок пока нет
- Original Papers: The Efficacy of Oral Ivermectin vs. Sulfur 10% Ointment For The Treatment of ScabiesДокумент8 страницOriginal Papers: The Efficacy of Oral Ivermectin vs. Sulfur 10% Ointment For The Treatment of ScabieserwinОценок пока нет
- Medical EntomologyДокумент39 страницMedical EntomologyRIZIQ TSОценок пока нет
- Analisis Perilaku Pencegahan Skabies Pada Santri Pondok Pesantren Nurul Huda Pringsewu LampungДокумент8 страницAnalisis Perilaku Pencegahan Skabies Pada Santri Pondok Pesantren Nurul Huda Pringsewu LampungSilviaОценок пока нет
- Tea Tree Oil Benefits, Uses and Potential Side Effects - Dr. AxeДокумент8 страницTea Tree Oil Benefits, Uses and Potential Side Effects - Dr. AxeJoseph TupasОценок пока нет
- What Is ScabiesДокумент7 страницWhat Is ScabiesKenОценок пока нет
- Jurnal Skabies EBM 2Документ18 страницJurnal Skabies EBM 2Bianti Nur'ainiОценок пока нет
- Medicines in BreastfeedingДокумент4 страницыMedicines in BreastfeedingIshan ShahОценок пока нет
- Absence of Responsible Member and Financial ConstraintsДокумент2 страницыAbsence of Responsible Member and Financial ConstraintsFavor ColaОценок пока нет