Вам также может понравиться
- Unusual Complications of Ultrasound Guided Central Venous CannulationДокумент4 страницыUnusual Complications of Ultrasound Guided Central Venous CannulationPrabakaran ParameswaranОценок пока нет
- Isccm PosterДокумент3 страницыIsccm PosterPrabakaran ParameswaranОценок пока нет
- Cirugi A Espan Ola: Meso-Cava Bypass As An Alternative To Multivisceral TransplantationДокумент2 страницыCirugi A Espan Ola: Meso-Cava Bypass As An Alternative To Multivisceral TransplantationHưng Nguyễn KiềuОценок пока нет
- Multimodality Cardiac Imaging of A Ventricular SepДокумент4 страницыMultimodality Cardiac Imaging of A Ventricular SephengkileonardОценок пока нет
- Image of The Month: Caput MedusaeДокумент1 страницаImage of The Month: Caput MedusaeRoery ImoetОценок пока нет
- Vascular Images: Endovascular Repair of Giant Bilateral Iliac Artery AneurysmДокумент2 страницыVascular Images: Endovascular Repair of Giant Bilateral Iliac Artery AneurysmKamil HannaОценок пока нет
- Hollehorst PlaquesДокумент3 страницыHollehorst PlaquesErick Roa GandicaОценок пока нет
- In Practice: Central Vein StenosisДокумент15 страницIn Practice: Central Vein Stenosisnilmania_01Оценок пока нет
- Symptomatic Central Venous Stenosis in A Hemodialysis Patient Leading To Loss of Arteriovenous Access: A Case Report and Literature ReviewДокумент5 страницSymptomatic Central Venous Stenosis in A Hemodialysis Patient Leading To Loss of Arteriovenous Access: A Case Report and Literature ReviewDivara SyautaОценок пока нет
- ABSTRACT TEVAR - Achmad Ismail S Putra NewДокумент3 страницыABSTRACT TEVAR - Achmad Ismail S Putra NewPutra AchmadОценок пока нет
- Tmp30e6 TMPДокумент4 страницыTmp30e6 TMPFrontiersОценок пока нет
- Acute Aortic Disecccion Type AДокумент15 страницAcute Aortic Disecccion Type AAnonymous envUOdVОценок пока нет
- CASE REPORT 3 - Acute Mesentric Venous Thrombosis With A History Recurrent DVT in Young Age A Case ReportДокумент2 страницыCASE REPORT 3 - Acute Mesentric Venous Thrombosis With A History Recurrent DVT in Young Age A Case Reportm.widodo190216Оценок пока нет
- Unusual Cardiac Complications of Staphylococcus: Aureus EndocarditisДокумент3 страницыUnusual Cardiac Complications of Staphylococcus: Aureus EndocarditisSara EslaitОценок пока нет
- Management of Chronic Venous Disease: 7th Annual Women's Heart & Vascular SymposiumДокумент3 страницыManagement of Chronic Venous Disease: 7th Annual Women's Heart & Vascular Symposiumatika5Оценок пока нет
- Revisión de Disección Celíaca y EsplénicaДокумент5 страницRevisión de Disección Celíaca y EsplénicaLuis AlfonsoОценок пока нет
- Left Hemothorax: Unusual Manifestation of Aortic DissectionДокумент5 страницLeft Hemothorax: Unusual Manifestation of Aortic DissectionIJAR JOURNALОценок пока нет
- Vol08 1 87-88strДокумент2 страницыVol08 1 87-88strAry-Adhi PutrantoОценок пока нет
- 4 2 - 181 182 PDFДокумент2 страницы4 2 - 181 182 PDFNam LeОценок пока нет
- AHAENDOCARDITEDEVICEДокумент18 страницAHAENDOCARDITEDEVICEAna MendelskiОценок пока нет
- Retained Catheter Fragment From A Fractured Tunneled Catheter-A Rare and Potentially Lethal ComplicationДокумент4 страницыRetained Catheter Fragment From A Fractured Tunneled Catheter-A Rare and Potentially Lethal ComplicationMahmoud DiaaОценок пока нет
- Hemodynamics and Diagnosis Venous Disease-Jvs 1207Документ21 страницаHemodynamics and Diagnosis Venous Disease-Jvs 1207Fahrudin ŠabanovićОценок пока нет
- Role of Embolization in The Management of Splenic Trauma: Case ReportДокумент3 страницыRole of Embolization in The Management of Splenic Trauma: Case ReportandreigustvОценок пока нет
- Insuficienta Venoasa CronicaДокумент15 страницInsuficienta Venoasa CronicaSimona IonitaОценок пока нет
- Acs 03 03 234Документ13 страницAcs 03 03 234IwanОценок пока нет
- Percutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial InfarctionДокумент4 страницыPercutaneous Coronary Intervention in A Patient With Severe Systemic Vasculitis and Myocardial Infarctionvam buddhaОценок пока нет
- Infectious Endo Carditis With Sub Aortic Diapharagma in A Patient With Coarctation of The AortaДокумент3 страницыInfectious Endo Carditis With Sub Aortic Diapharagma in A Patient With Coarctation of The AortaIJAR JOURNALОценок пока нет
- Acute Aortic Syndrome – More in The SpectruДокумент5 страницAcute Aortic Syndrome – More in The Spectrufabiola shoshajОценок пока нет
- New England Journal Medicine: The ofДокумент11 страницNew England Journal Medicine: The ofCyntia AndrinaОценок пока нет
- (Traves D. Crabtree) BRS Surgical Specialties PDFДокумент254 страницы(Traves D. Crabtree) BRS Surgical Specialties PDFCosmin Alexa100% (2)
- Inferior Mesenteric Arteriovenous Fistula With Ischemic Colitis: Multidetector Computed Tomographic Angiography For DiagnosisДокумент4 страницыInferior Mesenteric Arteriovenous Fistula With Ischemic Colitis: Multidetector Computed Tomographic Angiography For DiagnosisGordana PuzovicОценок пока нет
- 1 s2.0 S1930043321003083 MainДокумент5 страниц1 s2.0 S1930043321003083 MainSandra ArellanoОценок пока нет
- Aortic-Esophageal Fistula (AEF) - A Case ReportДокумент5 страницAortic-Esophageal Fistula (AEF) - A Case ReportWorld Journal of Case Reports and Clinical Images (ISSN: 2835-1568) CODEN:USAОценок пока нет
- Coronary Stent Infections A Case of Pericardial Abscess and Stent Displacement After Repeated PTCA Procedures Which Required An Emergency SurgeryДокумент4 страницыCoronary Stent Infections A Case of Pericardial Abscess and Stent Displacement After Repeated PTCA Procedures Which Required An Emergency SurgeryAthenaeum Scientific PublishersОценок пока нет
- Ruptured Abdominal Aortic Aneurysm in A Young Male PatientДокумент4 страницыRuptured Abdominal Aortic Aneurysm in A Young Male PatientKristanto Ayomi Ayomi AriОценок пока нет
- Tuberculous Aortitis An Extremely Rare Cause of Supra Aortic Trunks StenosisДокумент5 страницTuberculous Aortitis An Extremely Rare Cause of Supra Aortic Trunks StenosisAthenaeum Scientific PublishersОценок пока нет
- HemodialysisДокумент11 страницHemodialysisjuan_sioОценок пока нет
- Late, Acute Presentation of A Large Brachial Artery Aneurysm Following Ligation of A Brescia-Cimino Arteriovenous FistulaДокумент11 страницLate, Acute Presentation of A Large Brachial Artery Aneurysm Following Ligation of A Brescia-Cimino Arteriovenous FistulaYorazaki MaessaОценок пока нет
- Intervesnsi Stroke 1Документ9 страницIntervesnsi Stroke 1Zilbran BerontaxОценок пока нет
- Clinicopathological Study of Varicose Veins (Descriptive Study)Документ10 страницClinicopathological Study of Varicose Veins (Descriptive Study)Vlad DraculaОценок пока нет
- Nejm 2016 Mesenteric IschemiaДокумент11 страницNejm 2016 Mesenteric IschemiarisewfОценок пока нет
- 10 1056@NEJMra1503884 PDFДокумент10 страниц10 1056@NEJMra1503884 PDFmarselamgeОценок пока нет
- Ecr2011 C-0318Документ11 страницEcr2011 C-0318zulvaasОценок пока нет
- Endovascular en Herida de BalaДокумент3 страницыEndovascular en Herida de BalaVero CarpaniОценок пока нет
- Doppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesДокумент12 страницDoppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesAbraham PaulОценок пока нет
- Vascular Access HemodialysisДокумент19 страницVascular Access Hemodialysisplethoraldork100% (1)
- Aortic CoarctationДокумент4 страницыAortic CoarctationFrancois Donatien De SadeОценок пока нет
- WJC 7 765Документ12 страницWJC 7 765RamadhyanОценок пока нет
- Venous DiseaseДокумент50 страницVenous Diseaseعرفان رفعت پناهОценок пока нет
- Arteriovenous Access For HemodialysisДокумент11 страницArteriovenous Access For Hemodialysislakshminivas PingaliОценок пока нет
- Bojar PediatricДокумент123 страницыBojar PediatricLuqman AlwiОценок пока нет
- Comerota 2010Документ5 страницComerota 2010Jade GomitaОценок пока нет
- Belhajsoulami 2018Документ3 страницыBelhajsoulami 2018rédaОценок пока нет
- Hartley Final PDFДокумент16 страницHartley Final PDFAlexandriaJoОценок пока нет
- Journal of Cardiac Surgery - 2021 - Benetti - Coronary Artery Fistula Where Are We NowДокумент2 страницыJournal of Cardiac Surgery - 2021 - Benetti - Coronary Artery Fistula Where Are We NowMaricela GuzmanОценок пока нет
- Vascular AccessДокумент47 страницVascular AccessChenny MencianoОценок пока нет
- Advanced Endovascular Therapy of Aortic DiseaseОт EverandAdvanced Endovascular Therapy of Aortic DiseaseAlan B. LumsdenОценок пока нет
- Phlebology, Vein Surgery and Ultrasonography: Diagnosis and Management of Venous DiseaseОт EverandPhlebology, Vein Surgery and Ultrasonography: Diagnosis and Management of Venous DiseaseОценок пока нет
- Diabetes and Peripheral Vascular Disease: Diagnosis and ManagementОт EverandDiabetes and Peripheral Vascular Disease: Diagnosis and ManagementОценок пока нет
- Protein StructureДокумент10 страницProtein StructureSzekeres-Csiki KatalinОценок пока нет
- K, K and PH: Dr. C.S. Gasser's ExcellentДокумент9 страницK, K and PH: Dr. C.S. Gasser's ExcellentSzekeres-Csiki KatalinОценок пока нет
- Medtronic 630G Pump FDA User GuideДокумент312 страницMedtronic 630G Pump FDA User GuideSzekeres-Csiki KatalinОценок пока нет
- CBF 01 GuideДокумент3 страницыCBF 01 GuideSzekeres-Csiki KatalinОценок пока нет
- медицинаДокумент10 страницмедицинаDariaОценок пока нет
- LactationДокумент24 страницыLactationJenyl Bajado100% (1)
- CholangiocarcinomaДокумент9 страницCholangiocarcinomaloloalpsheidiОценок пока нет
- Editorial Board 2013 Journal of The American Academy of DermatologyДокумент1 страницаEditorial Board 2013 Journal of The American Academy of DermatologyYusmiatiОценок пока нет
- Neonatal Abstinence Syndrome Advances in Diagnosis and TreatmentДокумент14 страницNeonatal Abstinence Syndrome Advances in Diagnosis and TreatmentdzratsoОценок пока нет
- Z50 Transducer Ficha Tecnica SheetДокумент3 страницыZ50 Transducer Ficha Tecnica SheetMarcos CharmeloОценок пока нет
- Diabetic Neuropathies: The Nerve Damage of DiabetesДокумент12 страницDiabetic Neuropathies: The Nerve Damage of DiabetestaqiedaОценок пока нет
- Year 2 Dentistry Griffith University Instrument List 2018 - StudentДокумент8 страницYear 2 Dentistry Griffith University Instrument List 2018 - StudentAntonio HeОценок пока нет
- Thanatologi International 2007Документ37 страницThanatologi International 2007Paul LeeОценок пока нет
- Royal Crescent Practice Brocher 12pp March 2010 PrintДокумент12 страницRoyal Crescent Practice Brocher 12pp March 2010 PrintyarleyОценок пока нет
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthДокумент50 страницHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthShu Dizon100% (1)
- Midwifery Management of First Trimester Bleeding and Early Pregnancy LossДокумент17 страницMidwifery Management of First Trimester Bleeding and Early Pregnancy LossliopergonОценок пока нет
- Eacvi Recommendations Valvular Regurgitation Summary PDFДокумент34 страницыEacvi Recommendations Valvular Regurgitation Summary PDFstoicea_katalinОценок пока нет
- Hemorrhoids: What Are Hemorroids?Документ2 страницыHemorrhoids: What Are Hemorroids?Igor DemićОценок пока нет
- Voluson E10 BrochureДокумент8 страницVoluson E10 BrochureJavier VergaraОценок пока нет
- Femur Fractures in Children - Case PresentationДокумент22 страницыFemur Fractures in Children - Case PresentationChristian MicallefОценок пока нет
- A Study On Internal Fixation of Bimalleolar Ankle FracturesДокумент4 страницыA Study On Internal Fixation of Bimalleolar Ankle FracturesIOSRjournalОценок пока нет
- Mnemonic S NSGДокумент18 страницMnemonic S NSGohsnapitsleiОценок пока нет
- Acute Abdomen FinalДокумент105 страницAcute Abdomen FinalAizul AzmiОценок пока нет
- Maternal Breastfeeding SatisfactionДокумент66 страницMaternal Breastfeeding SatisfactionALisa ZaharaОценок пока нет
- Thoracic & Abdominal Wall BlocksДокумент57 страницThoracic & Abdominal Wall Blocksvignoth23112000Оценок пока нет
- Pemicu 2 Blok KGD Jovian LutfiДокумент77 страницPemicu 2 Blok KGD Jovian LutfiJovian LutfiОценок пока нет
- Professional ResumeДокумент1 страницаProfessional ResumeDouglas RutledgeОценок пока нет
- Congenital Talipes Equinovarus FinalДокумент28 страницCongenital Talipes Equinovarus FinalLakshmi Narayan R100% (2)
- NauseaДокумент2 страницыNauseaRomadhona KhoiriОценок пока нет
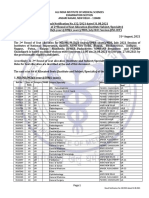
- 2nd Round Seat Allotment Result MDMS MDS Final NET2Документ52 страницы2nd Round Seat Allotment Result MDMS MDS Final NET2SARKAR JAVED AKHTARОценок пока нет
- Knee Ligament InjuriesДокумент5 страницKnee Ligament InjuriesNijin XmxОценок пока нет
- Agora ListДокумент61 страницаAgora ListVincent John Rigor100% (1)
- Cek List BiomedicДокумент159 страницCek List BiomedicIboedIstina100% (1)
- Anaesthesiology Case (Kaarthigan)Документ36 страницAnaesthesiology Case (Kaarthigan)Kaarthigan RamaiahОценок пока нет