Вам также может понравиться
- High-Expansion Foam Generators: Installation, Operation, and Maintenance ManualДокумент70 страницHigh-Expansion Foam Generators: Installation, Operation, and Maintenance Manualbenon100% (1)
- Fire and Other Emergency ProceduresДокумент17 страницFire and Other Emergency ProceduresbenonОценок пока нет
- Access To Information: Under Ontario's Information and Privacy ActsДокумент6 страницAccess To Information: Under Ontario's Information and Privacy ActsbenonОценок пока нет
- Prepared by F. S. Salla Ag. Commissioner of Fire Public Safety Division Fire and Rescue ForceДокумент19 страницPrepared by F. S. Salla Ag. Commissioner of Fire Public Safety Division Fire and Rescue ForcebenonОценок пока нет
- Rope Skills: Knots, Lashing and WhippingДокумент15 страницRope Skills: Knots, Lashing and WhippingbenonОценок пока нет
- Ppe and ScbaДокумент77 страницPpe and ScbabenonОценок пока нет
- Ind Fire BrigadeДокумент46 страницInd Fire Brigadebenon100% (1)
- South Dakota Certified: Rescue Operations (Technician) NFPA 1006, 2013Документ1 страницаSouth Dakota Certified: Rescue Operations (Technician) NFPA 1006, 2013benonОценок пока нет
- Ammonia and Urea Plants PDFДокумент48 страницAmmonia and Urea Plants PDFbenon100% (1)
- Wellington County Fire Training SCBA PresentationДокумент25 страницWellington County Fire Training SCBA PresentationbenonОценок пока нет
- Respirator References: - 29 CFR 1910.134 - ANSI Z88.2-1992Документ21 страницаRespirator References: - 29 CFR 1910.134 - ANSI Z88.2-1992benonОценок пока нет
- SCBA Training: Salem Fire Department ISI Viking Air Pack Training 2008Документ63 страницыSCBA Training: Salem Fire Department ISI Viking Air Pack Training 2008benonОценок пока нет
- Careers and Career Management - PPT 11Документ26 страницCareers and Career Management - PPT 11benonОценок пока нет
- Induction Training PDFДокумент51 страницаInduction Training PDFbenonОценок пока нет
- Ammonia Secondary Reforming: By: Gerard B. Hawkins Managing Director, CEOДокумент10 страницAmmonia Secondary Reforming: By: Gerard B. Hawkins Managing Director, CEObenonОценок пока нет
- This Course Has A Pre-Course Requirement That Must Be Completed by The Student. If The Student Does Not Complete The Pre-Course Requirement (Q0379), A Certificate Will Not Be IssuedДокумент3 страницыThis Course Has A Pre-Course Requirement That Must Be Completed by The Student. If The Student Does Not Complete The Pre-Course Requirement (Q0379), A Certificate Will Not Be IssuedbenonОценок пока нет
- Bpcl-Kochi Refinery: To The Hon. Jury Members of Safety Innovation Awards 2008-2009Документ62 страницыBpcl-Kochi Refinery: To The Hon. Jury Members of Safety Innovation Awards 2008-2009benonОценок пока нет
- Induction TrainingДокумент26 страницInduction TrainingbenonОценок пока нет
- Fire Extinguisher Monthly Checklist PDFДокумент1 страницаFire Extinguisher Monthly Checklist PDFbenonОценок пока нет
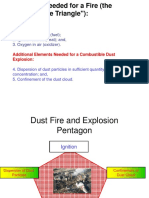
- Fire PentagonДокумент2 страницыFire PentagonbenonОценок пока нет
- Hand SafetyДокумент59 страницHand SafetybenonОценок пока нет
- A Devastating Fire: Amri HospitalДокумент18 страницA Devastating Fire: Amri HospitalbenonОценок пока нет
- Critical Levels For AmmoniaДокумент8 страницCritical Levels For AmmoniabenonОценок пока нет
- Ammonia Risk Assessment Laura Boles ENV385: Chemistry and Toxicology Instructor Muthu Kuchanur 02/04/2019Документ12 страницAmmonia Risk Assessment Laura Boles ENV385: Chemistry and Toxicology Instructor Muthu Kuchanur 02/04/2019benonОценок пока нет
- Experiment 8 Ammonia NitrogenДокумент6 страницExperiment 8 Ammonia NitrogenbenonОценок пока нет
- Ammonia Translocation in Cyanobactcria: Spirulina PlatensisДокумент14 страницAmmonia Translocation in Cyanobactcria: Spirulina PlatensisbenonОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Unit - 3 - 4 - QuestionsДокумент7 страницUnit - 3 - 4 - QuestionsCHETANMPATILОценок пока нет
- E-Recruitment: A Comparison With Traditional Recruitment and Selection ProcessДокумент4 страницыE-Recruitment: A Comparison With Traditional Recruitment and Selection ProcessArdina SovitasariОценок пока нет
- Management Theory Practice Ww45nXj6ReДокумент243 страницыManagement Theory Practice Ww45nXj6ResaumilshuklaОценок пока нет
- Department of Labor and Employment: Republic of The Philippines Intramuros, ManilaДокумент2 страницыDepartment of Labor and Employment: Republic of The Philippines Intramuros, ManilaElaine Fiona VillafuerteОценок пока нет
- ExecutionДокумент5 страницExecutionTiffany TewОценок пока нет
- 4 Makati Haberdashery Vs NLRC, Nov 15, 1989Документ6 страниц4 Makati Haberdashery Vs NLRC, Nov 15, 1989Perry YapОценок пока нет
- Metrolab Industries V ConfesorДокумент10 страницMetrolab Industries V ConfesorbrendamanganaanОценок пока нет
- Interview Appraisal FormДокумент4 страницыInterview Appraisal FormGaurav Narula100% (1)
- Management of The Internal Audit FunctionДокумент18 страницManagement of The Internal Audit FunctionJennylyn B. Sina-onОценок пока нет
- Presentation12 1Документ10 страницPresentation12 1api-345507444Оценок пока нет
- Precast Industry Guide 15-08-24Документ56 страницPrecast Industry Guide 15-08-24gemotorresОценок пока нет
- Staffing and Leading A Growing CompanyДокумент12 страницStaffing and Leading A Growing CompanyMaroden Sanchez GarciaОценок пока нет
- Case 1Документ1 страницаCase 1Lưu Hồng Hạnh 4KT-20ACNОценок пока нет
- Child Labour (Prohibition and Regulation) Amendment Bill, 2016Документ2 страницыChild Labour (Prohibition and Regulation) Amendment Bill, 2016Gowtham RainaОценок пока нет
- The Impact of Globalization On Industrial RelationsДокумент2 страницыThe Impact of Globalization On Industrial RelationsSharmistha MitraОценок пока нет
- Coaching and MentoringДокумент33 страницыCoaching and MentoringSiddharth ManuОценок пока нет
- Great Depression EssayДокумент34 страницыGreat Depression Essay纳尔 吉娜Оценок пока нет
- Presentation: On Recruitment and Selection Process in BPO SectorДокумент21 страницаPresentation: On Recruitment and Selection Process in BPO Sectornandini99sharmaОценок пока нет
- Child Labour - Simple English Wikipedia, The Free EncyclopediaДокумент2 страницыChild Labour - Simple English Wikipedia, The Free Encyclopediaapi-281088185Оценок пока нет
- 5S Meeting Attendance: Date: Time / Duration: Training Faculty: Program Covered: Methods and Tools UsedДокумент8 страниц5S Meeting Attendance: Date: Time / Duration: Training Faculty: Program Covered: Methods and Tools Usedsrinivasann1981Оценок пока нет
- Shan, CVДокумент4 страницыShan, CVShan ViswanathanОценок пока нет
- Due 3232 Unit 2Документ23 страницыDue 3232 Unit 2api-317626559Оценок пока нет
- Aim Approach To HRMДокумент11 страницAim Approach To HRMKAVYA SHANU K100% (1)
- An Overview of Urbanization and Structural Transformation in AfricaДокумент29 страницAn Overview of Urbanization and Structural Transformation in AfricaLarry KiptooОценок пока нет
- Employee Handbook RestaurantДокумент68 страницEmployee Handbook RestaurantJef S Adam100% (1)
- Abiodun Boluwatife ProjectДокумент53 страницыAbiodun Boluwatife ProjectAjeleye Shola TofunmiОценок пока нет
- SAQA US 15034 - Confined SpaceДокумент3 страницыSAQA US 15034 - Confined Spacejacobus_louw4329Оценок пока нет
- Skema Audit InternalДокумент4 страницыSkema Audit InternaligoeneezmОценок пока нет
- Motivate PeopleДокумент1 страницаMotivate PeoplemrajisОценок пока нет
- HSSE ManagerДокумент1 страницаHSSE ManagerJose PollardОценок пока нет