Вам также может понравиться
- RoB 2.0 Guidance Parallel TrialДокумент68 страницRoB 2.0 Guidance Parallel TrialOscar PonceОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- 361 2012 LaHayeДокумент9 страниц361 2012 LaHayeOscar PonceОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Loss To Follow-UpДокумент11 страницLoss To Follow-UpOscar PonceОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Advance 1079 Patel 2007Документ12 страницAdvance 1079 Patel 2007Oscar PonceОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- 2018 JAMA Random Effects MA Serguiou StylianosДокумент2 страницы2018 JAMA Random Effects MA Serguiou StylianosOscar PonceОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Testosterone Replacement Therapy and Components of The Metabolic SyndromeДокумент11 страницTestosterone Replacement Therapy and Components of The Metabolic SyndromeOscar PonceОценок пока нет
- Ven A Mi - Arautos Do ReiДокумент5 страницVen A Mi - Arautos Do ReiOscar PonceОценок пока нет
- Final Trial of Thesis The Following Are The Basis For This Trial Upload A Document UnderstandДокумент1 страницаFinal Trial of Thesis The Following Are The Basis For This Trial Upload A Document UnderstandOscar PonceОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Terapi CompressionДокумент10 страницTerapi CompressionErlinda KarimОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- BNSL-040-B3 Practical Block 3Документ130 страницBNSL-040-B3 Practical Block 3Pawan ShokeenОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Prevenção de Trauma Perineal Revisão Cochranne 2017Документ89 страницPrevenção de Trauma Perineal Revisão Cochranne 2017Francine XavierОценок пока нет
- PROTOCOLO - Nursing Swallow Screen ProtocolДокумент2 страницыPROTOCOLO - Nursing Swallow Screen ProtocolAldo Hip NaranjoОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Serviciile Sociale in Situatii de RiscДокумент15 страницServiciile Sociale in Situatii de RiscAlina HoaraОценок пока нет
- Evidence Based Dietetics PracticeДокумент11 страницEvidence Based Dietetics PracticeLinaTrisnawatiОценок пока нет
- Case of Grade 4 Bedsore Over Sacral Region With Management A Case ReportДокумент3 страницыCase of Grade 4 Bedsore Over Sacral Region With Management A Case ReportAmna AliОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Nurse Resume Masters Degree TemplateДокумент2 страницыNurse Resume Masters Degree TemplatehenryodomОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Textbook of Neural Repair and Rehabilitation Medical Neurorehabilitation 2006Документ802 страницыTextbook of Neural Repair and Rehabilitation Medical Neurorehabilitation 2006enigelОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Skinny Gut Diet by Brenda Watson - ExcerptДокумент24 страницыSkinny Gut Diet by Brenda Watson - ExcerptCrown Publishing Group56% (9)
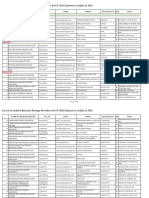
- List of Notified Bodies Under Directive - 93-42 EEC Medical DevicesДокумент332 страницыList of Notified Bodies Under Directive - 93-42 EEC Medical DevicesJamal MohamedОценок пока нет
- Patient Rights & Responsibilities 03 Aug 2011Документ1 страницаPatient Rights & Responsibilities 03 Aug 2011Jv SinghОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- ADHDДокумент17 страницADHDapi-3822433Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
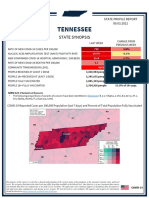
- Tennessee State Profile Report 20210903 PublicДокумент17 страницTennessee State Profile Report 20210903 PublicAnonymous GF8PPILW5Оценок пока нет
- VET0811 SeДокумент6 страницVET0811 SeterrywinkleОценок пока нет
- Bacteria and Immune Defenses: Helicobacter PyloriДокумент4 страницыBacteria and Immune Defenses: Helicobacter PyloriMary Rose SJ JimenezОценок пока нет
- IEM MinutesДокумент5 страницIEM Minutesprasad.dhruv91Оценок пока нет
- Coding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1Документ1 страницаCoding Poli Mata: Papillitis H46 Hypertension Ocular:h40.0 Macula H35.8 Ptosis H02.4 Chalazion H00.1 Asthenopia H53.1nurcasanОценок пока нет
- SBLE English SimpleДокумент8 страницSBLE English SimpleKian GonzagaОценок пока нет
- Health - Questions - Pdf-Igcse Biology WorksheetДокумент22 страницыHealth - Questions - Pdf-Igcse Biology WorksheetPrincess KimОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Lesson Plan Emergency NursingДокумент41 страницаLesson Plan Emergency NursingSwapnil Mahapure100% (1)
- Will The Speed of COVID-19-vaccine Development Reset Industry NormsДокумент7 страницWill The Speed of COVID-19-vaccine Development Reset Industry NormsraytjanОценок пока нет
- KONSULTA 073123 v1Документ124 страницыKONSULTA 073123 v1Substationsix MalaboncpsОценок пока нет
- Therapeutic Guidelines in Systemic Fungal Infection. 3rd Ed.Документ127 страницTherapeutic Guidelines in Systemic Fungal Infection. 3rd Ed.PrisОценок пока нет
- NCM 107 Module 2M Ethico Moral Aspects of NursingДокумент18 страницNCM 107 Module 2M Ethico Moral Aspects of NursingTrisha ApillanesОценок пока нет
- Data Change Template CardivaДокумент123 страницыData Change Template CardivaNorilyn FloresОценок пока нет
- WHO MHGap Guide English PDFДокумент121 страницаWHO MHGap Guide English PDFYolanda Dwi OktaviyaniОценок пока нет
- Case Report Eye Emergency RoomДокумент10 страницCase Report Eye Emergency RoomBangkit Benedikta HutchersonОценок пока нет
- The Impact of Drug Abuse On Society A Review On Drug Abuse in The Context of SocietyДокумент3 страницыThe Impact of Drug Abuse On Society A Review On Drug Abuse in The Context of SocietyInternational Journal of Innovative Science and Research TechnologyОценок пока нет
- Temporomandibular Joint Syndrome PDFДокумент4 страницыTemporomandibular Joint Syndrome PDFMaxim BzoviiОценок пока нет