Вам также может понравиться
- Diagnosis of Endometrial Biopsies and Curettings: A Practical ApproachОт EverandDiagnosis of Endometrial Biopsies and Curettings: A Practical ApproachОценок пока нет
- Modified FIGOSystems 1 and 2 For 2018 IJGOДокумент17 страницModified FIGOSystems 1 and 2 For 2018 IJGOMariana HernandezОценок пока нет
- Practical Gynecologic Pathology: Frequently Asked QuestionsОт EverandPractical Gynecologic Pathology: Frequently Asked QuestionsJian-Jun WeiОценок пока нет
- Modified FIGOSystems 1 and 2 For 2018 IJGOДокумент17 страницModified FIGOSystems 1 and 2 For 2018 IJGOISAH D. CONTORAОценок пока нет
- Practical Lymph Node and Bone Marrow Pathology: Frequently Asked QuestionsОт EverandPractical Lymph Node and Bone Marrow Pathology: Frequently Asked QuestionsEndi WangОценок пока нет
- Distribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemДокумент3 страницыDistribution of Causes of Abnormal Uterine Bleeding Using The New FIGO Classification SystemirmaarmiyahОценок пока нет
- Best Practice Issue On "Abnormal Uterine Bleeding"Документ21 страницаBest Practice Issue On "Abnormal Uterine Bleeding"Rosu GeorgeОценок пока нет
- AUB 2012 SSDSDDDDDDDDДокумент7 страницAUB 2012 SSDSDDDDDDDDPitra Mukhlis WardaniОценок пока нет
- Abnormal Uterine Bleeding Research ProtocolДокумент21 страницаAbnormal Uterine Bleeding Research Protocoljananiravi.2003Оценок пока нет
- FIGO Classification System PALM-COEIN For Causes oДокумент12 страницFIGO Classification System PALM-COEIN For Causes oEdwin SondakhОценок пока нет
- Hamerlynck2018 Article FertilityOutcomeAfterTreatmentДокумент7 страницHamerlynck2018 Article FertilityOutcomeAfterTreatmentMahida El shafiОценок пока нет
- Abnormal Uterine Bleeding in Reproductive-Age Women - Terminology and PALM-COEIN Etiology Classification - UpToDateДокумент46 страницAbnormal Uterine Bleeding in Reproductive-Age Women - Terminology and PALM-COEIN Etiology Classification - UpToDateCristinaCaprosОценок пока нет
- CE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFДокумент5 страницCE (Vi) F (SK) PF1 (PS OM) PFA (SS) PN (SS) PDFrizqina ajraОценок пока нет
- 168 05 06 - Ragusa PDFДокумент10 страниц168 05 06 - Ragusa PDFSeptian WidiantoОценок пока нет
- 2816aub PDFДокумент6 страниц2816aub PDFIbrahim AbdullahОценок пока нет
- ArticleДокумент16 страницArticleobbyОценок пока нет
- Biomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueДокумент12 страницBiomarkers in Abnormal Uterine Bleeding: Precision Medicine in Assisted Reproductive Technologies Special IssueWahyuning PutriОценок пока нет
- Abnormal Uterine Bleeding in Perimenopausal WomenДокумент15 страницAbnormal Uterine Bleeding in Perimenopausal WomenOrchid LandОценок пока нет
- Shah2021 Article WhatHappensAfterRandomisedContДокумент10 страницShah2021 Article WhatHappensAfterRandomisedContJulián Cabezas PeñaОценок пока нет
- AUB ManagementДокумент18 страницAUB ManagementSteve EmmanuelОценок пока нет
- CID en EmbarazadaДокумент10 страницCID en EmbarazadaCristian MuñozОценок пока нет
- Antepartum Hemorrhage PDFДокумент23 страницыAntepartum Hemorrhage PDFfrizkapfОценок пока нет
- 2019 Article 505Документ12 страниц2019 Article 505Xiomara Alfaro AraujoОценок пока нет
- The FIGO Systems For Nomenclature and Classification of Causes of Abnormal Uterine Bleeding in The Reproductive YearsДокумент7 страницThe FIGO Systems For Nomenclature and Classification of Causes of Abnormal Uterine Bleeding in The Reproductive YearsAurielle Annalicia SetiawanОценок пока нет
- Guidelines of Investigations of Premenopausal Women With Abnormal Uterine Bleeding - 2020Документ6 страницGuidelines of Investigations of Premenopausal Women With Abnormal Uterine Bleeding - 2020cara0319Оценок пока нет
- Literature Review of Postpartum HaemorrhageДокумент4 страницыLiterature Review of Postpartum Haemorrhagegxkswirif100% (1)
- Guideline On Investigations of Premenopausal Women With Abnormal Uterine BleedingДокумент8 страницGuideline On Investigations of Premenopausal Women With Abnormal Uterine Bleedingvera ditaОценок пока нет
- Abnormal Uterine Bleeding in Reproductive-Age Patients: FIGO System 1 Terminology and Symptoms and SДокумент2 страницыAbnormal Uterine Bleeding in Reproductive-Age Patients: FIGO System 1 Terminology and Symptoms and SMariana HernandezОценок пока нет
- Meconium-Stained Amniotic Fluid: A Risk Factor For Postpartum HemorrhageДокумент5 страницMeconium-Stained Amniotic Fluid: A Risk Factor For Postpartum HemorrhagelaniОценок пока нет
- The Diagnostic Criteria For Chronic EndometritisДокумент7 страницThe Diagnostic Criteria For Chronic EndometritisyuriescaidaОценок пока нет
- AUB Classification - FIGOДокумент8 страницAUB Classification - FIGOjeansabalosОценок пока нет
- A Study To Correlate Clinical With Pathological Findings in Abnormal Uterine Bleeding (AUB)Документ9 страницA Study To Correlate Clinical With Pathological Findings in Abnormal Uterine Bleeding (AUB)goodnotes.pdfОценок пока нет
- Figo Palm CoeinДокумент8 страницFigo Palm CoeinemptylotОценок пока нет
- The Paris System For Reporting Urinary CytologyДокумент9 страницThe Paris System For Reporting Urinary Cytologyrafasp.arqtОценок пока нет
- Intl J Gynecology Obste - 2022 - Munro - The FIGO Ovulatory Disorders Classification SystemДокумент20 страницIntl J Gynecology Obste - 2022 - Munro - The FIGO Ovulatory Disorders Classification SystemMinerba MelendrezОценок пока нет
- Nejmoa 2303966Документ11 страницNejmoa 2303966Raul ForjanОценок пока нет
- Evidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFДокумент16 страницEvidence-Based Guidelines For The Management of Abnormally Invasive Placenta Recommendations From The International PDFErika GuerreroОценок пока нет
- A Retrospective Study of Maternal and Perinatal Outcome in Patients of Postpartum Haemorrhage in A Tertiary Care HospitalДокумент5 страницA Retrospective Study of Maternal and Perinatal Outcome in Patients of Postpartum Haemorrhage in A Tertiary Care HospitalAdzana Yasadhy Hangga PrasetyoОценок пока нет
- Critically Ill Obstetric Patients and Feto-Maternal Outcome: EditorialДокумент3 страницыCritically Ill Obstetric Patients and Feto-Maternal Outcome: EditorialMahtosurup GodavarthyОценок пока нет
- JPM 12 01098 v2Документ11 страницJPM 12 01098 v2Rizki FebriyaniОценок пока нет
- Ijgo 12687 PDFДокумент6 страницIjgo 12687 PDFDjlatino LatinoОценок пока нет
- Pelvic Organ Prolapse After Laparoscopic Hysterectomy Compared With Vaginal Hysterectomy: The POP-UP StudyДокумент10 страницPelvic Organ Prolapse After Laparoscopic Hysterectomy Compared With Vaginal Hysterectomy: The POP-UP Studymuhammadnurul asmiОценок пока нет
- Abnormal Uterine BleedingДокумент12 страницAbnormal Uterine BleedingGilang DermawanОценок пока нет
- Jurnal Hiperplasia EndometriumДокумент5 страницJurnal Hiperplasia Endometriumperussi pranadiptaОценок пока нет
- IJHS Robson PublicationДокумент9 страницIJHS Robson PublicationVinod BharatiОценок пока нет
- Hang Tuah Medical Journal: Wardani, HTMJ Volume 15 No 1 2017Документ10 страницHang Tuah Medical Journal: Wardani, HTMJ Volume 15 No 1 2017Gufron MustofaОценок пока нет
- Antepartum HaemorrhageДокумент23 страницыAntepartum HaemorrhageSutanti Lara DewiОценок пока нет
- Ectopic PregnancyДокумент24 страницыEctopic PregnancybertouwОценок пока нет
- A Systeatic Review N Meta AnalysisДокумент16 страницA Systeatic Review N Meta Analysisheni fitriyantiОценок пока нет
- Investigation and Management of MenorrhagiaДокумент26 страницInvestigation and Management of MenorrhagiaRahdin Ahmad Faresy Al-HamidiОценок пока нет
- 1 s2.0 S1028455917303273 PDFДокумент2 страницы1 s2.0 S1028455917303273 PDFRachmad SammuliaОценок пока нет
- 10 1111@jog 143436777777Документ17 страниц10 1111@jog 143436777777Epiphany SonderОценок пока нет
- Classification/staging Systems For Endometriosis: The State of The ArtДокумент9 страницClassification/staging Systems For Endometriosis: The State of The ArtMerlin MuktialiОценок пока нет
- Clinical Practice Guidelines For Recurrent Miscarriage in High-Income Countries: A Systematic ReviewДокумент26 страницClinical Practice Guidelines For Recurrent Miscarriage in High-Income Countries: A Systematic ReviewshashankiswaitingОценок пока нет
- Medip, IJRCOG-8374 OДокумент6 страницMedip, IJRCOG-8374 Oalaesa2007Оценок пока нет
- Jurnal 8Документ11 страницJurnal 8salsabela fithriОценок пока нет
- Bakker 2012Документ10 страницBakker 2012ieoОценок пока нет
- Sistema de ParisДокумент177 страницSistema de ParisNabor Gallo100% (1)
- Correcting Data For Case Mix in Stroke Medicine: Unplanned Deliveries, PillДокумент2 страницыCorrecting Data For Case Mix in Stroke Medicine: Unplanned Deliveries, PillNatanael SusantoОценок пока нет
- JCM 12 06175Документ10 страницJCM 12 06175Taulant MukaОценок пока нет
- Family MapДокумент1 страницаFamily MapNur Vicka VickaОценок пока нет
- Urinary Tract Infection in Children: Diagnosis, Treatment, Imaging - Comparison of Current GuidelinesДокумент8 страницUrinary Tract Infection in Children: Diagnosis, Treatment, Imaging - Comparison of Current GuidelinesNur Vicka VickaОценок пока нет
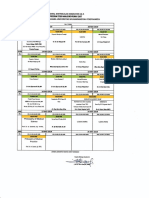
- Jadwal Matrikulasi 16 AДокумент1 страницаJadwal Matrikulasi 16 ANur Vicka VickaОценок пока нет
- Journal AppraisalДокумент1 страницаJournal AppraisalNur Vicka VickaОценок пока нет
- Comparison of Growth Pattern in Neonates On Breast Feed Versus Formula FeedДокумент14 страницComparison of Growth Pattern in Neonates On Breast Feed Versus Formula FeedNur Vicka VickaОценок пока нет
- Mms Health Recovery Guidebook 1 October 2016Документ346 страницMms Health Recovery Guidebook 1 October 2016omar hazard94% (50)
- Histologia, Conceitos Básicos Dos Tecidos - GitiranaДокумент13 страницHistologia, Conceitos Básicos Dos Tecidos - GitiranaJhonnatam EliasОценок пока нет
- Registrars Manual On Band DДокумент32 страницыRegistrars Manual On Band DkailasasundaramОценок пока нет
- WRAS MarinasДокумент4 страницыWRAS MarinasAdam ReesОценок пока нет
- UrethralstricturesДокумент37 страницUrethralstricturesNinaОценок пока нет
- Nahom ShewangizawДокумент38 страницNahom Shewangizawawel centerОценок пока нет
- Book of Best Practices Trauma and The Role of Mental Health in Post-Conflict RecoveryДокумент383 страницыBook of Best Practices Trauma and The Role of Mental Health in Post-Conflict RecoveryDiego Salcedo AvilaОценок пока нет
- MODULE 8: Settings, Processes, Methods, and Tools in Social WorkДокумент4 страницыMODULE 8: Settings, Processes, Methods, and Tools in Social WorkAlexandra Nicole RugaОценок пока нет
- Alprazolam: Why Is This Medicine Prescribed To You?Документ1 страницаAlprazolam: Why Is This Medicine Prescribed To You?Jerome GeronimoОценок пока нет
- Tano Vs SocratesДокумент3 страницыTano Vs SocratesNimpa PichayОценок пока нет
- Nah Incarcerated HerniaДокумент4 страницыNah Incarcerated Herniafelix_the_meowОценок пока нет
- XA6 - Emergency Provision Workbook 2020 v0 - 5 - CKДокумент35 страницXA6 - Emergency Provision Workbook 2020 v0 - 5 - CKguyОценок пока нет
- English Teacher's NotesДокумент24 страницыEnglish Teacher's NotesPrincess KimОценок пока нет
- Cold Cryotherapy NotesДокумент6 страницCold Cryotherapy Notesakheel ahammedОценок пока нет
- SHARON SCHULTZ, ET AL. v. JANOS GUOTH, M.D. AND KHALED F. RABIE, M.D. (Parish of Rapides)Документ18 страницSHARON SCHULTZ, ET AL. v. JANOS GUOTH, M.D. AND KHALED F. RABIE, M.D. (Parish of Rapides)wstОценок пока нет
- Nso AblaparotomyДокумент3 страницыNso AblaparotomyAleeya SarajanОценок пока нет
- Infant Tub RationaleДокумент4 страницыInfant Tub RationaleAllen Kenneth PacisОценок пока нет
- Anti ParasiteДокумент4 страницыAnti ParasiteVörös Bálint100% (1)
- Septic System Design ManualДокумент31 страницаSeptic System Design ManualtonyОценок пока нет
- Paper On Rag PickersДокумент11 страницPaper On Rag PickershsrapsОценок пока нет
- Validity and Reliability Study of The Turkish Version of Ego Identity Process QuestionairreДокумент6 страницValidity and Reliability Study of The Turkish Version of Ego Identity Process QuestionairreSergio F. GonzalezОценок пока нет
- 2022 Projects City of BethlehemДокумент17 страниц2022 Projects City of BethlehemLVNewsdotcomОценок пока нет
- Postharvest Technology-Importance: Eufemio G. Barcelon, PHDДокумент56 страницPostharvest Technology-Importance: Eufemio G. Barcelon, PHDJohanna Amor L. AdaoОценок пока нет
- Example: Write Sentences To Give Advice. Use The Verb and The Information in Parenthesis. (1.25 Points)Документ2 страницыExample: Write Sentences To Give Advice. Use The Verb and The Information in Parenthesis. (1.25 Points)Robert Jesús Guerrero GilerОценок пока нет
- CircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesДокумент43 страницыCircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesMenaОценок пока нет
- LimpДокумент7 страницLimpRakesh DudiОценок пока нет
- Viroguard Sanitizer SDS-WatermartДокумент7 страницViroguard Sanitizer SDS-WatermartIshara VithanaОценок пока нет
- Physical Fitness Test Individual Score CardДокумент12 страницPhysical Fitness Test Individual Score CardJunessa TadinaОценок пока нет
- BMI W HFA Validated (3!24!2017)Документ151 страницаBMI W HFA Validated (3!24!2017)jeffordillasОценок пока нет
- COUNCIL DIRECTIVE 90 269 EEC On The Minimum Health and Safety Requirements For The Manual Handling of LoadsДокумент7 страницCOUNCIL DIRECTIVE 90 269 EEC On The Minimum Health and Safety Requirements For The Manual Handling of Loadsromedic36Оценок пока нет
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)От EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Рейтинг: 3 из 5 звезд3/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (30)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionОт EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionРейтинг: 4 из 5 звезд4/5 (404)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (3)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (81)
- The Marshmallow Test: Mastering Self-ControlОт EverandThe Marshmallow Test: Mastering Self-ControlРейтинг: 4.5 из 5 звезд4.5/5 (60)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 4 из 5 звезд4/5 (4)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (5)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (170)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (46)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Empath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainОт EverandEmpath: The Survival Guide For Highly Sensitive People: Protect Yourself From Narcissists & Toxic Relationships. Discover How to Stop Absorbing Other People's PainРейтинг: 4 из 5 звезд4/5 (95)
- Manipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesОт EverandManipulation: The Ultimate Guide To Influence People with Persuasion, Mind Control and NLP With Highly Effective Manipulation TechniquesРейтинг: 4.5 из 5 звезд4.5/5 (1412)