Вам также может понравиться
- Concise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryОт EverandConcise Guide to Clinical Dentistry: Common Prescriptions In Clinical DentistryОценок пока нет
- Flowchart I Dan TДокумент2 страницыFlowchart I Dan TfauzanОценок пока нет
- Studies in OphthalmologyДокумент17 страницStudies in OphthalmologyMuhammad Usman Ghani GormaniОценок пока нет
- Treatment of TB in Adults: by Dr. Irfhan Ali Hyder AliДокумент45 страницTreatment of TB in Adults: by Dr. Irfhan Ali Hyder AliInspireGutsОценок пока нет
- New Drugs and Regimens for TB: 2015 UpdateДокумент21 страницаNew Drugs and Regimens for TB: 2015 UpdateNop PiromОценок пока нет
- VeIP GU TESДокумент6 страницVeIP GU TESMohan KumarОценок пока нет
- Burn Education Module 2.14.22Документ22 страницыBurn Education Module 2.14.22Ashraf HusseinОценок пока нет
- Sinha2021 Article SteroidSensitiveNephroticSyndrДокумент21 страницаSinha2021 Article SteroidSensitiveNephroticSyndrMrinmayeeDeshmukhОценок пока нет
- Steroid Sensitive Nephrotic Syndrome - Indian Guidelines-1Документ55 страницSteroid Sensitive Nephrotic Syndrome - Indian Guidelines-1Tushar AmbedareОценок пока нет
- Presentations Codeine Scheduling Workshops Brisbane 13 December 2017 02Документ45 страницPresentations Codeine Scheduling Workshops Brisbane 13 December 2017 02Bruno FernandesОценок пока нет
- Intermittent Versus Continuous Systemic Therapy For Metastatic Colorectal CancerДокумент34 страницыIntermittent Versus Continuous Systemic Therapy For Metastatic Colorectal CanceraritrisnawatiОценок пока нет
- (2006) ALTINER, D. D Et Al. Comparison of Weekly and Daily Incremental Protocols of Narrowband Ultraviolet B Phototherapy For PsoriasisДокумент5 страниц(2006) ALTINER, D. D Et Al. Comparison of Weekly and Daily Incremental Protocols of Narrowband Ultraviolet B Phototherapy For PsoriasisCassandra VérasОценок пока нет
- Vabysmo PrescribingДокумент16 страницVabysmo PrescribingMahesh PalaniОценок пока нет
- Suspected COVID-19 Cases Management in Triage HospitalsДокумент6 страницSuspected COVID-19 Cases Management in Triage HospitalsMuhamed RamadanОценок пока нет
- INJartesunate 60mg Booklet ENGДокумент6 страницINJartesunate 60mg Booklet ENGElly PetroОценок пока нет
- Studies Summary in OphthalmologyДокумент12 страницStudies Summary in OphthalmologyMuhammad Usman Ghani GormaniОценок пока нет
- Clinical Guideline for Managing Periorbital Cellulitis in ChildrenДокумент5 страницClinical Guideline for Managing Periorbital Cellulitis in ChildrenJohn M. HemsworthОценок пока нет
- Adolescentes BFM HyperCVAD alacacioglu2015Документ5 страницAdolescentes BFM HyperCVAD alacacioglu2015erickmattosОценок пока нет
- AAO 2015 Atropine For Myopia DR Donald Tan 11-16-15 RedactedДокумент15 страницAAO 2015 Atropine For Myopia DR Donald Tan 11-16-15 RedactedunonounoОценок пока нет
- Magli Oc Co 2006Документ4 страницыMagli Oc Co 2006lisnallОценок пока нет
- Use of Aeds in 2011 and Beyond: Optimizing Clinical ManagementДокумент32 страницыUse of Aeds in 2011 and Beyond: Optimizing Clinical ManagementchandanОценок пока нет
- Opioid Topic DiscussionДокумент22 страницыOpioid Topic Discussionapi-587439953Оценок пока нет
- Asma 101Документ43 страницыAsma 101Asfiksia NeonatorumОценок пока нет
- Management of Retinoblastoma With Extraocular Tumour ExtensionДокумент2 страницыManagement of Retinoblastoma With Extraocular Tumour ExtensionkarinarakhmaОценок пока нет
- Tb Guideline TreatmentДокумент19 страницTb Guideline TreatmentRana Ahsan JavedОценок пока нет
- Leukemia Treatment Regimens 7937Документ3 страницыLeukemia Treatment Regimens 7937Irfan FathurrahmanОценок пока нет
- New May2020 PDFДокумент7 страницNew May2020 PDFDoctorMoodyОценок пока нет
- AkdkfjakdkssДокумент5 страницAkdkfjakdkssYogi SaputraОценок пока нет
- TB and Leprosy Case Management Desk Guide - 3rd Edition - 22 - 2 - 2019Документ7 страницTB and Leprosy Case Management Desk Guide - 3rd Edition - 22 - 2 - 2019Bigabwa BernardОценок пока нет
- 5 - Treatment of Drug Susceptible TB v01132020Документ18 страниц5 - Treatment of Drug Susceptible TB v01132020RHU MinalabacОценок пока нет
- TB Diagnosis and TreatmentДокумент2 страницыTB Diagnosis and TreatmentFermin K. CuasitoОценок пока нет
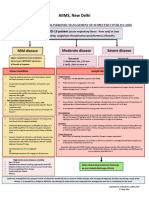
- AIIMS Syndromic ApproachДокумент1 страницаAIIMS Syndromic ApproachRagul VОценок пока нет
- Journal Reading OphtalmologyДокумент17 страницJournal Reading Ophtalmologytiara nadya putriandaОценок пока нет
- MX Protocol Book FinalДокумент42 страницыMX Protocol Book FinalPawan ChoudharyОценок пока нет
- Ema-Co Gy GTDДокумент4 страницыEma-Co Gy GTDTowhidulIslamОценок пока нет
- 596 Ifosfamide Etoposide Ie TherapyДокумент6 страниц596 Ifosfamide Etoposide Ie Therapyravindra0504090Оценок пока нет
- Davis Symposium AdvancesInSarcomaДокумент55 страницDavis Symposium AdvancesInSarcomaFernando SilalahiОценок пока нет
- NEL/NCL BRVO Pathway: (Box A) Anti-VEGF (Box B) SteroidДокумент1 страницаNEL/NCL BRVO Pathway: (Box A) Anti-VEGF (Box B) SteroidElika Dwi CahyaniОценок пока нет
- TB and Leprosy Case Management Desk GuideДокумент7 страницTB and Leprosy Case Management Desk GuideBigabwa BernardОценок пока нет
- EVS Study Guide for Bacterial EndophthalmitisДокумент7 страницEVS Study Guide for Bacterial EndophthalmitisRasha Mounir Abdel-Kader El-TanamlyОценок пока нет
- RX LTBI Adults Without HIV Infection - UpToDateДокумент2 страницыRX LTBI Adults Without HIV Infection - UpToDateDylanОценок пока нет
- HypophosphataemiaДокумент4 страницыHypophosphataemiaLütfiye ÖzlemОценок пока нет
- Preopanc Trial - PancreasДокумент20 страницPreopanc Trial - PancreasRajalakshmi RadhakrishnanОценок пока нет
- Communicable Disease Nursing Part II Diseases (1) 2Документ21 страницаCommunicable Disease Nursing Part II Diseases (1) 2MK LiОценок пока нет
- Edited: DR - Dairion Gatot M.Ked SP - PD-KHOMДокумент57 страницEdited: DR - Dairion Gatot M.Ked SP - PD-KHOMayuhati siregarОценок пока нет
- Medical Affairs Concept Sheet - MACS - For Investigator Initiated Trials - Part 1 IS - FIN EdДокумент8 страницMedical Affairs Concept Sheet - MACS - For Investigator Initiated Trials - Part 1 IS - FIN EdNadira ErynaОценок пока нет
- CD Summary UpdatedДокумент27 страницCD Summary UpdatedOPERAñA ELLAYZA RB DECANOОценок пока нет
- BCCA Protocol for DOXOrubicin - Ifosfamide - Mesna ChemoДокумент4 страницыBCCA Protocol for DOXOrubicin - Ifosfamide - Mesna ChemoHep PutОценок пока нет
- Visual Acuity Outcomes and Anti–Vascular Endothelial Growth Factor Therapy Intensity in Neovascular Age-Related Macular Degeneration Patients A Real-World Analysis of 49 485 EyesДокумент12 страницVisual Acuity Outcomes and Anti–Vascular Endothelial Growth Factor Therapy Intensity in Neovascular Age-Related Macular Degeneration Patients A Real-World Analysis of 49 485 EyesmaleticjОценок пока нет
- Uterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorДокумент32 страницыUterine Sarcoma - Pharmacologic Management - Cancer Therapy AdvisorIrfan FathurrahmanОценок пока нет
- Abnoba ViscumДокумент44 страницыAbnoba ViscumAlexandre Funcia100% (1)
- Radiation PleisotherapyДокумент33 страницыRadiation PleisotherapyBavadharaniОценок пока нет
- Tuberculosis Treatment GuideДокумент30 страницTuberculosis Treatment GuideIbrahim JeldiОценок пока нет
- DetoxДокумент4 страницыDetoxShahrul Nizan HashimОценок пока нет
- Prevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati UpadhyayДокумент42 страницыPrevention & Treatment of Rop: Presentation: DR Manaswinee Sahoo Guide: DR Swati Upadhyaypranaya mallОценок пока нет
- YERVOY Annex I Summary of Product CharacteristicsДокумент65 страницYERVOY Annex I Summary of Product CharacteristicsGag PafОценок пока нет
- COMMUNICABLE DISEASE NURSING (Part II: Diseases)Документ21 страницаCOMMUNICABLE DISEASE NURSING (Part II: Diseases)ROBERT C. REÑA, BSN, RN, MAN (ue)88% (34)
- Trigeminal Neuralgia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandTrigeminal Neuralgia, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- A Simple Guide to Myasthenia Gravis (Updated), Diagnosis, Treatment and Related ConditionsОт EverandA Simple Guide to Myasthenia Gravis (Updated), Diagnosis, Treatment and Related ConditionsОценок пока нет
- Minipro Lampiran 3 Data KuesionerДокумент3 страницыMinipro Lampiran 3 Data KuesionerfauzanОценок пока нет
- Lembar Soap Neo FadilДокумент1 страницаLembar Soap Neo FadilfauzanОценок пока нет
- Pembimbing: Dr. Gita Sekar Prihanti, M.PD - KedДокумент8 страницPembimbing: Dr. Gita Sekar Prihanti, M.PD - KedfauzanОценок пока нет
- InfusДокумент29 страницInfusfauzanОценок пока нет
- Atherosclerosis: Magdalena Mika, Renata B. Kostogrys, Magdalena Franczyk - Zar Ow, Agnieszka Wikiera, Edyta Ma SlakДокумент6 страницAtherosclerosis: Magdalena Mika, Renata B. Kostogrys, Magdalena Franczyk - Zar Ow, Agnieszka Wikiera, Edyta Ma SlakfauzanОценок пока нет
- JOURNAL READING KhalishahДокумент7 страницJOURNAL READING KhalishahfauzanОценок пока нет
- Gagal Ginjal KronikДокумент29 страницGagal Ginjal KronikfauzanОценок пока нет
- Daftar PustakaДокумент1 страницаDaftar PustakafauzanОценок пока нет
- Atherosclerosis: Magdalena Mika, Renata B. Kostogrys, Magdalena Franczyk - Zar Ow, Agnieszka Wikiera, Edyta Ma SlakДокумент6 страницAtherosclerosis: Magdalena Mika, Renata B. Kostogrys, Magdalena Franczyk - Zar Ow, Agnieszka Wikiera, Edyta Ma SlakfauzanОценок пока нет
- Daftar Singkatan: PJK Penyakit Jantung KoronerДокумент1 страницаDaftar Singkatan: PJK Penyakit Jantung KoronerfauzanОценок пока нет
- 9 Autism Spectrum2Документ29 страниц9 Autism Spectrum2fauzanОценок пока нет
- Format Pomr WordДокумент2 страницыFormat Pomr WordfauzanОценок пока нет
- ResepДокумент1 страницаResepfauzanОценок пока нет
- 2Документ8 страниц2fauzanОценок пока нет
- PAR-Q Physical Activity Readiness QuestionnaireДокумент3 страницыPAR-Q Physical Activity Readiness QuestionnaireMhervin BisisОценок пока нет
- 23 Nov 2022Документ1 страница23 Nov 2022Tahir ShahОценок пока нет
- Colposcopy 2Документ29 страницColposcopy 2Prabhakar SrinivasanОценок пока нет
- 100 Papers in Clinical Psychiatry Psychosomatic Medicine Malingering in The Medical Setting.Документ18 страниц100 Papers in Clinical Psychiatry Psychosomatic Medicine Malingering in The Medical Setting.J. M. SolisОценок пока нет
- Chitoglucan New OverviewДокумент6 страницChitoglucan New OverviewmjmorcelliОценок пока нет
- Mental Health ResourcesДокумент5 страницMental Health ResourcesAnna R ZahorОценок пока нет
- Tumbuhan Biji Terbuka (Gymnospermae) Dan Tertutup (Angiospermae)Документ10 страницTumbuhan Biji Terbuka (Gymnospermae) Dan Tertutup (Angiospermae)novianti InnaОценок пока нет
- The Big Four by Rolf GordonДокумент40 страницThe Big Four by Rolf GordonArcanistОценок пока нет
- Chapter 2. Nutritional Requirements and Food Based Dietary Guidelines Study Questions 2 (SQ 2)Документ2 страницыChapter 2. Nutritional Requirements and Food Based Dietary Guidelines Study Questions 2 (SQ 2)Julie Amor ZantuaОценок пока нет
- Hashimoto ThyroiditisДокумент6 страницHashimoto Thyroiditismananginsiang100% (1)
- Dr. Aakash Harakhchand Shah's Clinic TeleconsultationДокумент1 страницаDr. Aakash Harakhchand Shah's Clinic TeleconsultationAnkeshОценок пока нет
- Gun Control PowerpointДокумент11 страницGun Control Powerpointapi-319208107Оценок пока нет
- Congestive Heart Failure NCPДокумент6 страницCongestive Heart Failure NCPShaira Ann Calamba100% (1)
- SCARED Form ScoringДокумент1 страницаSCARED Form ScoringKaty PuiuОценок пока нет
- ResearchДокумент20 страницResearchapi-413279928Оценок пока нет
- Acute Sinusitis Diagnosis and TreatmentДокумент27 страницAcute Sinusitis Diagnosis and Treatment1720209111Оценок пока нет
- Bias and Confounding: Nayana FernandoДокумент31 страницаBias and Confounding: Nayana FernandoanojОценок пока нет
- INITIAL DATA BASE Form For Family 1Документ5 страницINITIAL DATA BASE Form For Family 1Reignallienn Inocencio MartinОценок пока нет
- Nepal Development Update Post Pandemic Nepal Charting A Resilient Recovery and Future Growth Directions PDFДокумент62 страницыNepal Development Update Post Pandemic Nepal Charting A Resilient Recovery and Future Growth Directions PDFSanjeev PradhanОценок пока нет
- Obstetrics 4Документ9 страницObstetrics 4Darrel Allan MandiasОценок пока нет
- Knowledge, Attitude and Practice of Cervical Cancer Screening Through Visual Inspection With Acetic AcidДокумент10 страницKnowledge, Attitude and Practice of Cervical Cancer Screening Through Visual Inspection With Acetic AcidIJPHSОценок пока нет
- Medikolegal Swamedikasi PenyakitДокумент8 страницMedikolegal Swamedikasi PenyakitMiftahul JannahОценок пока нет
- BSBWHS401 - Implement and Monitor WHS Policies, Procedures and Programs To Meet Legislative RequirementsДокумент11 страницBSBWHS401 - Implement and Monitor WHS Policies, Procedures and Programs To Meet Legislative RequirementsPattaniya KosayothinОценок пока нет
- CHMM Exam Blueprint Details Hazardous Materials Management Certification RequirementsДокумент2 страницыCHMM Exam Blueprint Details Hazardous Materials Management Certification RequirementswoowangsiОценок пока нет
- University of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundДокумент7 страницUniversity of Caloocan City: Bachelor of Arts Major in Political Science The Problem and Its BackgroundJericko Perez AvilaОценок пока нет
- 485 5032 Assignment 1 Greenwich University PassДокумент27 страниц485 5032 Assignment 1 Greenwich University PassThy ThơОценок пока нет
- Types of fitness activities and modifiable risk factorsДокумент14 страницTypes of fitness activities and modifiable risk factorsMaria Cristy CanceranОценок пока нет
- Wilfredo Mallari Resume Safety Supervisor UpdatedДокумент1 страницаWilfredo Mallari Resume Safety Supervisor Updatedwilly mallariОценок пока нет
- Mammograms and Other Breast Imaging Procedures: What Is A Mammogram?Документ25 страницMammograms and Other Breast Imaging Procedures: What Is A Mammogram?Marina StosicОценок пока нет
- Learning Activities. I Box A Difficulties of Frontliners Amidst Covid 19 Impact of Social Media in Student Cause and Effect of Online LearningДокумент2 страницыLearning Activities. I Box A Difficulties of Frontliners Amidst Covid 19 Impact of Social Media in Student Cause and Effect of Online LearningChristine Mae BoleaОценок пока нет