Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Training The Power PitcherДокумент11 страницTraining The Power PitcherRodulfo AlvaradoОценок пока нет
- Applied Physiology For TennisДокумент6 страницApplied Physiology For TennisRodulfo AlvaradoОценок пока нет
- Athletes at High AltitudeДокумент7 страницAthletes at High AltitudeRodulfo AlvaradoОценок пока нет
- A Coaches Dozen 12 Fundamental Principles For.13Документ3 страницыA Coaches Dozen 12 Fundamental Principles For.13Rodulfo AlvaradoОценок пока нет
- C ProgrammingДокумент205 страницC ProgrammingSrinivasan RamachandranОценок пока нет
- V Ships Appln FormДокумент6 страницV Ships Appln Formkaushikbasu2010Оценок пока нет
- Numerical Solution of Ordinary Differential EquationsДокумент31 страницаNumerical Solution of Ordinary Differential Equationschandu3072002100% (1)
- 6 The Periodization TrainingДокумент24 страницы6 The Periodization TrainingRodulfo Alvarado100% (1)
- Audit AP TestsДокумент3 страницыAudit AP TestsSweet Emme100% (1)
- Action Anticipation and Motor Resonance in Elite Basketball PlayersДокумент8 страницAction Anticipation and Motor Resonance in Elite Basketball PlayersRodulfo AlvaradoОценок пока нет
- A Clustered Repeated-Sprint Running Protocol For Team-Sport Athletes Performed in Normobaric HypoxiaДокумент7 страницA Clustered Repeated-Sprint Running Protocol For Team-Sport Athletes Performed in Normobaric HypoxiaRodulfo AlvaradoОценок пока нет
- The Journal of Strength and Conditioning Research Volume 23 Issue 6 2009 (Doi 10.1519/jsc.0b013e3181b3df32) Zagatto, Alessandro M Beck, Wladimir R Gobatto, Claudio A - Validity of The Running Ana PDFДокумент8 страницThe Journal of Strength and Conditioning Research Volume 23 Issue 6 2009 (Doi 10.1519/jsc.0b013e3181b3df32) Zagatto, Alessandro M Beck, Wladimir R Gobatto, Claudio A - Validity of The Running Ana PDFAlienzОценок пока нет
- Advancing Hypoxic Training in Team SportsДокумент9 страницAdvancing Hypoxic Training in Team SportsRodulfo AlvaradoОценок пока нет
- A Clustered Repeated-Sprint Running Protocol For Team-Sport Athletes Performed in Normobaric HypoxiaДокумент7 страницA Clustered Repeated-Sprint Running Protocol For Team-Sport Athletes Performed in Normobaric HypoxiaRodulfo AlvaradoОценок пока нет
- Analysis and Testing For BasketballДокумент8 страницAnalysis and Testing For BasketballRodulfo AlvaradoОценок пока нет
- AOSSM Early Sport Specialization Consensus StatementДокумент8 страницAOSSM Early Sport Specialization Consensus StatementRodulfo AlvaradoОценок пока нет
- A New Strategy For The Implementation of An Aerobic Exercise SessionДокумент7 страницA New Strategy For The Implementation of An Aerobic Exercise SessionRodulfo AlvaradoОценок пока нет
- The Yo Yo Intermittent Recovery Test inДокумент7 страницThe Yo Yo Intermittent Recovery Test inRodulfo AlvaradoОценок пока нет
- Mod. 34 Classic Compact T06Документ4 страницыMod. 34 Classic Compact T06Jaime Li AliОценок пока нет
- Flexural Analysis of Beams (Part 2)Документ7 страницFlexural Analysis of Beams (Part 2)Johnnette Nafuerza AggabaoОценок пока нет
- LinkedIn Learning - Workplace Learning Report 2021 EN 1Документ65 страницLinkedIn Learning - Workplace Learning Report 2021 EN 1Ronald FriasОценок пока нет
- WFP-Remote Household Food Security Survey Brief-Sri Lanka Aug 2022Документ18 страницWFP-Remote Household Food Security Survey Brief-Sri Lanka Aug 2022Adaderana OnlineОценок пока нет
- Proforma Invoice: DescriptionДокумент3 страницыProforma Invoice: Descriptionanon-690278Оценок пока нет
- BSHM 23 ReviewerДокумент8 страницBSHM 23 ReviewerTrixie Mae MuncadaОценок пока нет
- Trusted Cloud Computing by Helmut Krcmar, Ralf Reussner, Bernhard Rumpe (Eds.)Документ335 страницTrusted Cloud Computing by Helmut Krcmar, Ralf Reussner, Bernhard Rumpe (Eds.)Hari HaranОценок пока нет
- Gild PitchДокумент19 страницGild PitchtejabharathОценок пока нет
- Uvas CaractДокумент10 страницUvas CaractgondeluОценок пока нет
- Attribute Achievement FormДокумент15 страницAttribute Achievement FormMiguel MenesesОценок пока нет
- Interviews: Personal Interview. Advantages and Disadvantages Business Is Largely A Social PhenomenonДокумент8 страницInterviews: Personal Interview. Advantages and Disadvantages Business Is Largely A Social PhenomenonSanjeev JayaratnaОценок пока нет
- Chapter 20: Sleep Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionДокумент4 страницыChapter 20: Sleep Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuОценок пока нет
- Job Interview CV TipsДокумент2 страницыJob Interview CV TipsCarlos Moraga Copier100% (1)
- MRI Week3 - Signal - Processing - TheoryДокумент43 страницыMRI Week3 - Signal - Processing - TheoryaboladeОценок пока нет
- Electronic Throttle ControlДокумент67 страницElectronic Throttle Controlmkisa70100% (1)
- Future War in Cities Alice Hills PDFДокумент5 страницFuture War in Cities Alice Hills PDFazardarioОценок пока нет
- Ajwin Handbuch enДокумент84 страницыAjwin Handbuch enEnzo AguilarОценок пока нет
- Investigation Report on Engine Room Fire on Ferry BerlinДокумент63 страницыInvestigation Report on Engine Room Fire on Ferry Berlin卓文翔Оценок пока нет
- Mumbai Tourist Attractions.Документ2 страницыMumbai Tourist Attractions.Guru SanОценок пока нет
- Fundamental of Computer MCQ: 1. A. 2. A. 3. A. 4. A. 5. A. 6. AДокумент17 страницFundamental of Computer MCQ: 1. A. 2. A. 3. A. 4. A. 5. A. 6. AacercОценок пока нет
- Water 07 02314Документ36 страницWater 07 02314Satyajit ShindeОценок пока нет
- Chapter 9 Lease DecisionsДокумент51 страницаChapter 9 Lease Decisionsceoji25% (4)
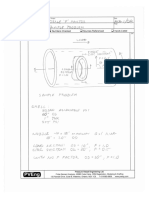
- Nozzle F Factor CalculationsДокумент5 страницNozzle F Factor CalculationsSivateja NallamothuОценок пока нет
- Cross-Sectional Tomography: Oral and Maxillofacial RadiologyДокумент7 страницCross-Sectional Tomography: Oral and Maxillofacial RadiologyPhanQuangHuyОценок пока нет
- 457 PDFДокумент8 страниц457 PDFAbbey Joy CollanoОценок пока нет
- Pakage PAU (Fruits)Документ70 страницPakage PAU (Fruits)Gary Bhullar57% (7)