Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- 160 GMAT PREP RC Passages - Official AnswersДокумент180 страниц160 GMAT PREP RC Passages - Official AnswersjanuanuОценок пока нет
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesДокумент4 страницыChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZОценок пока нет
- Clio Prosecutor Resolution FinalДокумент4 страницыClio Prosecutor Resolution FinalGabby ElardoОценок пока нет
- Clio Prosecutor Resolution ExamДокумент3 страницыClio Prosecutor Resolution ExamGabby ElardoОценок пока нет
- BLOCK 2 GROUP D (For The Wife) S.Y. 2020-2021 Mercader, Aiza A. Oarde, Anthea Margarita R. Ocampo, Clio Marie Bernadette CДокумент4 страницыBLOCK 2 GROUP D (For The Wife) S.Y. 2020-2021 Mercader, Aiza A. Oarde, Anthea Margarita R. Ocampo, Clio Marie Bernadette CGabby ElardoОценок пока нет
- Sales Agreement Draft (Oven)Документ2 страницыSales Agreement Draft (Oven)Gabby ElardoОценок пока нет
- CIR Vs Filinvest Development CorpoДокумент18 страницCIR Vs Filinvest Development CorpoGabby ElardoОценок пока нет
- Practice of Profession Samahan NG Optometrists Sa Pilipinas v. Acebedo International Corporation G.R. No. 117097. March 21, 1997. FactsДокумент1 страницаPractice of Profession Samahan NG Optometrists Sa Pilipinas v. Acebedo International Corporation G.R. No. 117097. March 21, 1997. FactsGabby ElardoОценок пока нет
- United Church of Christ in The Philippines Vs Bradford - ElardoДокумент1 страницаUnited Church of Christ in The Philippines Vs Bradford - ElardoGabby ElardoОценок пока нет
- Article 34 Amendment by RA 8042Документ4 страницыArticle 34 Amendment by RA 8042Gabby ElardoОценок пока нет
- Case 123 CMC ACE Vs LaguesmaДокумент1 страницаCase 123 CMC ACE Vs LaguesmaGabby ElardoОценок пока нет
- Atty. Viviana M. PaguiriganДокумент1 страницаAtty. Viviana M. PaguiriganGabby ElardoОценок пока нет
- ELARDO, SEBASTIAN GABRIEL M. (Illegal Recruitment)Документ7 страницELARDO, SEBASTIAN GABRIEL M. (Illegal Recruitment)Gabby ElardoОценок пока нет
- Amorito V. Canete For Petitioner. Pablo R. Cruz For Private RespondentДокумент5 страницAmorito V. Canete For Petitioner. Pablo R. Cruz For Private RespondentGabby ElardoОценок пока нет
- Review Outline in AgencyДокумент6 страницReview Outline in AgencyGabby ElardoОценок пока нет
- Natres Digest Pool 2Документ11 страницNatres Digest Pool 2Gabby ElardoОценок пока нет
- Martin B. Laurea and Associates For Petitioner-Appellee. Office of The Solicitor General For Respondents-AppellantsДокумент5 страницMartin B. Laurea and Associates For Petitioner-Appellee. Office of The Solicitor General For Respondents-AppellantsGabby ElardoОценок пока нет
- Merida vs. PeopleДокумент2 страницыMerida vs. PeopleGabby ElardoОценок пока нет
- ELARDO, SEBASTIAN GABRIEL M. (Illegal Recruitment)Документ23 страницыELARDO, SEBASTIAN GABRIEL M. (Illegal Recruitment)Gabby ElardoОценок пока нет
- Abe-Abe Vs MantaДокумент4 страницыAbe-Abe Vs MantaGabby ElardoОценок пока нет
- Page - 1Документ94 страницыPage - 1Dayan Cabriga100% (1)
- Vol24no5 Pdf-Version PDFДокумент152 страницыVol24no5 Pdf-Version PDFPuspaОценок пока нет
- Chap2 (Partial)Документ8 страницChap2 (Partial)Tannie Lyn Ebarle BasubasОценок пока нет
- Dengue FeverДокумент39 страницDengue FeverMuhammad Alauddin Sarwar100% (15)
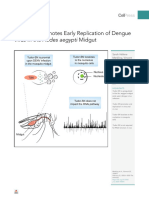
- Pi Is 2589004220300547Документ27 страницPi Is 2589004220300547valdirbrazsОценок пока нет
- Task 1 Read the text below. Match choices (А-Н) to (1-5) - There are three choices you do not need to use. Write your answers on the separate answer sheetДокумент7 страницTask 1 Read the text below. Match choices (А-Н) to (1-5) - There are three choices you do not need to use. Write your answers on the separate answer sheetNazar KuzivОценок пока нет
- Skripsi Full Tanpa Bab PembahasanДокумент80 страницSkripsi Full Tanpa Bab PembahasanAndre BinsarОценок пока нет
- Science - July 8, 2022 USAДокумент144 страницыScience - July 8, 2022 USASimej100% (1)
- Beijing Pledges Further Support To Laos: Vientiane TimesДокумент28 страницBeijing Pledges Further Support To Laos: Vientiane TimesNaughty VongОценок пока нет
- Mikroorganisma Dan Kesannya Terhadap Benda Hidup: Microorganisms and Their Effects On Living ThingsДокумент33 страницыMikroorganisma Dan Kesannya Terhadap Benda Hidup: Microorganisms and Their Effects On Living Thingsmiss amieyОценок пока нет
- FadfdДокумент5 страницFadfdVanessa MeanaОценок пока нет
- QR Dengue Infection PDF Final PDFДокумент8 страницQR Dengue Infection PDF Final PDFina2407jrОценок пока нет
- JEE: Chapter Notes and Important Question of Inverse Trigonometric FunctionsДокумент15 страницJEE: Chapter Notes and Important Question of Inverse Trigonometric FunctionsPrashant HuddarОценок пока нет
- OPLAN: Limpyo Ug DaubДокумент47 страницOPLAN: Limpyo Ug DaubtwirldleОценок пока нет
- Vaccine Access and Hesitancy: The Public Health Importance of VaccinesДокумент30 страницVaccine Access and Hesitancy: The Public Health Importance of VaccinesJmarie Brillantes PopiocoОценок пока нет
- Math Final Pre TestДокумент13 страницMath Final Pre TestJames Patrick ValenciaОценок пока нет
- WHO Dengue Classification and Case Management-FlyerДокумент2 страницыWHO Dengue Classification and Case Management-FlyerKathleen DyОценок пока нет
- Fever Sfi Dhs 2016Документ17 страницFever Sfi Dhs 2016hafnisashameenОценок пока нет
- Data Rawat Inap2Документ152 страницыData Rawat Inap2Muhammad Aqiem MuttaqinОценок пока нет
- Science Lesson Plan Dengue Jigsaw-2Документ5 страницScience Lesson Plan Dengue Jigsaw-2Devi RambaranОценок пока нет
- CHN DOH ProgramsДокумент158 страницCHN DOH Programsjudd wilson100% (1)
- Knowledge, Attitude and Practices For Dengue ControlДокумент26 страницKnowledge, Attitude and Practices For Dengue ControlCASY31Оценок пока нет
- Dengue PreventionДокумент20 страницDengue PreventionSharath WankdothОценок пока нет
- MR Dengue BrochureДокумент8 страницMR Dengue Brochureapi-322658380Оценок пока нет
- CITY STAR Newspaper March 25 - April 25 EditionДокумент20 страницCITY STAR Newspaper March 25 - April 25 Editioncity star newspaperОценок пока нет
- Usg For DBDДокумент5 страницUsg For DBDhappy gummyОценок пока нет
- Task 2Документ8 страницTask 2Chin Jia YiОценок пока нет
- Communicable Disease QuizДокумент2 страницыCommunicable Disease QuizPlacida Mequiabas National High SchoolОценок пока нет