Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Rojas - Et - Al. - 2013.efficacy of A Cognitive Intervention Program in Patients With Mild Cognitive ImpairmentДокумент7 страницRojas - Et - Al. - 2013.efficacy of A Cognitive Intervention Program in Patients With Mild Cognitive ImpairmentSu AjaОценок пока нет
- Castellanos 2011 Alteration and ReorganizationДокумент13 страницCastellanos 2011 Alteration and ReorganizationSu AjaОценок пока нет
- Self Consciousness ScaleДокумент11 страницSelf Consciousness ScaleSu AjaОценок пока нет
- Niu2010.Cognitive Stimulation Therapy in The Treatment of Neuropsychiatric Symptoms in Alzheimer's Disease - A Randomized Controlled TrialДокумент10 страницNiu2010.Cognitive Stimulation Therapy in The Treatment of Neuropsychiatric Symptoms in Alzheimer's Disease - A Randomized Controlled TrialSu AjaОценок пока нет
- Bokde, 2006.functional Connectivity of The Fusiform Gyrus During A Face-Matching Task in Subjects With MCI PDFДокумент12 страницBokde, 2006.functional Connectivity of The Fusiform Gyrus During A Face-Matching Task in Subjects With MCI PDFSu AjaОценок пока нет
- Cellulite: A Review of Its Physiology and TreatmentДокумент6 страницCellulite: A Review of Its Physiology and TreatmentShanna MitchellОценок пока нет
- Can Musical Training Influence Brain ConnectivityДокумент24 страницыCan Musical Training Influence Brain ConnectivityJohan NuñezОценок пока нет
- Papp, 2009.immediate and Delayed Effects of Co PDFДокумент11 страницPapp, 2009.immediate and Delayed Effects of Co PDFSu AjaОценок пока нет
- Van Os-2015-Cognitive Interventions in Older PДокумент14 страницVan Os-2015-Cognitive Interventions in Older PSu AjaОценок пока нет
- Mills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentДокумент19 страницMills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentSu AjaОценок пока нет
- Mills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentДокумент10 страницMills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentSu AjaОценок пока нет
- Mills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentДокумент19 страницMills & Tamnes, 2014.methods and Considerations For Longitudinal Structural Brain Imaging Analysis Across DevelopmentSu AjaОценок пока нет
- Bottiroli2008.Long-term Effects of Memory Training in The Elderly - A Longitudinal StudyДокумент13 страницBottiroli2008.Long-term Effects of Memory Training in The Elderly - A Longitudinal StudySu AjaОценок пока нет
- Engvig, 2012.hippocampal Subfield Volumes Correlate With Memory Training Benefit in Subjective Memory Impairment PDFДокумент7 страницEngvig, 2012.hippocampal Subfield Volumes Correlate With Memory Training Benefit in Subjective Memory Impairment PDFSu AjaОценок пока нет
- ArticolДокумент17 страницArticolMinodora MilenaОценок пока нет
- Astle-2015-Cognitive Training Enhances IntrinsДокумент7 страницAstle-2015-Cognitive Training Enhances IntrinsSu AjaОценок пока нет
- Egvig, 2014..effects of Cognitive Training On GДокумент14 страницEgvig, 2014..effects of Cognitive Training On GSu AjaОценок пока нет
- Bahar Fuchs 2013 Cognitive Training and CognitДокумент14 страницBahar Fuchs 2013 Cognitive Training and CognitSu AjaОценок пока нет
- Takeuchi-2010-Training of Working Memory Impac PDFДокумент7 страницTakeuchi-2010-Training of Working Memory Impac PDFSu AjaОценок пока нет
- Snarski-2011-The Effects of Behavioral Activat PDFДокумент9 страницSnarski-2011-The Effects of Behavioral Activat PDFSu AjaОценок пока нет
- Egvig, 2014..effects of Cognitive Training On GДокумент13 страницEgvig, 2014..effects of Cognitive Training On GSu AjaОценок пока нет
- Belleville 2011 Training Related Brain PlasticДокумент12 страницBelleville 2011 Training Related Brain PlasticSu AjaОценок пока нет
- Takeuchi-2010-Training of Working Memory ImpacДокумент16 страницTakeuchi-2010-Training of Working Memory ImpacSu AjaОценок пока нет
- Nozawa-2015-Effects of Different Types of CognДокумент18 страницNozawa-2015-Effects of Different Types of CognSu AjaОценок пока нет
- Rodakowski 2015 Non Pharmacological InterventiДокумент16 страницRodakowski 2015 Non Pharmacological InterventiSu AjaОценок пока нет
- Bamidis, 2014.a Review of Physical and Cognitive Interventions in Aging.Документ15 страницBamidis, 2014.a Review of Physical and Cognitive Interventions in Aging.Su AjaОценок пока нет
- NIH Public AccessДокумент23 страницыNIH Public AccessSu AjaОценок пока нет
- Styliadis-2015-Neuroplastic Effects of CombineДокумент12 страницStyliadis-2015-Neuroplastic Effects of CombineSu AjaОценок пока нет
- Sala Llonch 2015 Reorganization of Brain NetwoДокумент11 страницSala Llonch 2015 Reorganization of Brain NetwoSu AjaОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Test Bank For Evolution 2nd Edition Media Update by Carl T Bergstrom Lee Alan Dugatkin Full DownloadДокумент14 страницTest Bank For Evolution 2nd Edition Media Update by Carl T Bergstrom Lee Alan Dugatkin Full Downloadaaronwarrenpgozeainyq100% (25)
- (L1 Biotechnology - Principles & Processes - PrinciplesДокумент65 страниц(L1 Biotechnology - Principles & Processes - PrinciplesOmar GillОценок пока нет
- Sched and CodesДокумент1 страницаSched and CodesCyriz Matthew MontesОценок пока нет
- Abstrak LaporanДокумент14 страницAbstrak LaporanAmaliah Putry PratiwiОценок пока нет
- Pertemuan 10&11. Linkage, CROSSING OVER, and Recombination PDFДокумент31 страницаPertemuan 10&11. Linkage, CROSSING OVER, and Recombination PDFDamar GreengoblinОценок пока нет
- Developmental Biology of The MeningesДокумент26 страницDevelopmental Biology of The MeningesI'Jaz Farritz MuhammadОценок пока нет
- Test 1Документ14 страницTest 1Phương LinhОценок пока нет
- Targeting WNT Signaling in Cancer Opportunities Abound If We Can Avoid The Sword of DamoclesДокумент300 страницTargeting WNT Signaling in Cancer Opportunities Abound If We Can Avoid The Sword of DamoclesGris CortezОценок пока нет
- Wainwright M. Life Comes From Space. The Decisive Evidence 2023Документ233 страницыWainwright M. Life Comes From Space. The Decisive Evidence 2023Attila SebőkОценок пока нет
- Soalan Peperiksaan Percubaan Sem 3 PahangДокумент8 страницSoalan Peperiksaan Percubaan Sem 3 PahangwanmarianiОценок пока нет
- Application of Tissue Culture Techniques in PotatoДокумент18 страницApplication of Tissue Culture Techniques in Potatokang_eebОценок пока нет
- Dwnload Full Concepts of Genetics 10th Edition Klug Test Bank PDFДокумент35 страницDwnload Full Concepts of Genetics 10th Edition Klug Test Bank PDFmaryjomacklemus100% (13)
- Environment Climate Plant and Vegetation Growth 2020Документ696 страницEnvironment Climate Plant and Vegetation Growth 2020Om BaronОценок пока нет
- BioHL P2 M04 TZ2Документ10 страницBioHL P2 M04 TZ2Chintia UtomoОценок пока нет
- Edexcel History A Level Coursework Civil RightsДокумент7 страницEdexcel History A Level Coursework Civil Rightsafiwftfbu100% (2)
- BiologyДокумент4 страницыBiologyNusrat HafeezОценок пока нет
- HUMSS2125 Trends, Networks and Critical Thinking in The 21st Century Culture Q2 Long Quiz 1 (Performance Task 1) - Attempt Review (20) 1Документ7 страницHUMSS2125 Trends, Networks and Critical Thinking in The 21st Century Culture Q2 Long Quiz 1 (Performance Task 1) - Attempt Review (20) 1PR-CUZZAMU STEVE CARL B.Оценок пока нет
- Ramzan Timetable Grade IX-AДокумент1 страницаRamzan Timetable Grade IX-AMBJОценок пока нет
- CYJS-16-45-85 (Alters Soil Microbial Populations To Facilitate Its Own Growth)Документ8 страницCYJS-16-45-85 (Alters Soil Microbial Populations To Facilitate Its Own Growth)JuanManuelAmaroLuisОценок пока нет
- Reading 3 - AdditionalДокумент4 страницыReading 3 - AdditionalDai NgoОценок пока нет
- Phycology UsamaДокумент8 страницPhycology UsamaUsama Shafiq Usama ShafiqОценок пока нет
- Budding Summative Assessment Jimena DueñasДокумент6 страницBudding Summative Assessment Jimena DueñasJimena DueñasОценок пока нет
- Guide To Nucleic Acid Purification-2Документ6 страницGuide To Nucleic Acid Purification-2DolphingОценок пока нет
- Mic 211 Lec 1Документ49 страницMic 211 Lec 1إسراء رمضانОценок пока нет
- Ap Bio Cricket LabДокумент5 страницAp Bio Cricket Labapi-197995289Оценок пока нет
- What Is The Difference Between Ingroup and Outgroup in BiologyДокумент2 страницыWhat Is The Difference Between Ingroup and Outgroup in BiologyJerico linderoОценок пока нет
- Syllabus 01242022Документ3 страницыSyllabus 01242022Amoya CОценок пока нет
- Stakeholders' Preferences On Production Forest Management: A Case Study in Forest District of BogorДокумент18 страницStakeholders' Preferences On Production Forest Management: A Case Study in Forest District of BogorMini Cool Bachdim-bieberОценок пока нет
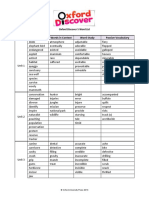
- Od Word List Level 5Документ7 страницOd Word List Level 5karyee limОценок пока нет
- Development of Teeth: January 2018Документ13 страницDevelopment of Teeth: January 2018Tesa RafkhaniОценок пока нет