Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
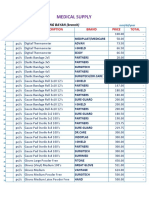
- Medical Supplies, & Baby Products PricelistДокумент5 страницMedical Supplies, & Baby Products PricelistParmasya Ng Bayan Bacolor Main BranchОценок пока нет
- Exam 3 Name: BSC 1011: Rhizopus?Документ7 страницExam 3 Name: BSC 1011: Rhizopus?Ariel FosterОценок пока нет
- CultureCoin Preparation Procedure For Miri Time-Lapse IncubatorДокумент2 страницыCultureCoin Preparation Procedure For Miri Time-Lapse IncubatorernestoveigaОценок пока нет
- Art Dynamic Morphology and Embryology PDFДокумент42 страницыArt Dynamic Morphology and Embryology PDFimageorge13Оценок пока нет
- BBBДокумент4 страницыBBBBoris ShalomovОценок пока нет
- Topic: 'Hiv and Aids'': Sub-Topic: Mode of TransmissionДокумент16 страницTopic: 'Hiv and Aids'': Sub-Topic: Mode of TransmissionwesterОценок пока нет
- Copy-Induced Breeding in FishДокумент31 страницаCopy-Induced Breeding in Fishhafiz anasОценок пока нет
- Disenfranchised Grief 10.22Документ20 страницDisenfranchised Grief 10.22dofiajoijОценок пока нет
- Mce Igcse Biology PPT c17Документ28 страницMce Igcse Biology PPT c17elaineОценок пока нет
- Binary FissionДокумент2 страницыBinary Fissionsajal aggarwalОценок пока нет
- Male Reproductive SystemДокумент19 страницMale Reproductive SystemAli JafriОценок пока нет
- Induced Breeding 2Документ3 страницыInduced Breeding 2Narasimha MurthyОценок пока нет
- Sissy Forum2Документ6 страницSissy Forum2Ali NasirОценок пока нет
- Artificial InseminationДокумент29 страницArtificial InseminationMayuri VohraОценок пока нет
- Tiger Fact SheetДокумент4 страницыTiger Fact Sheetparasara66Оценок пока нет
- Lab Manual Animal Systematic II 2017 - Activity IДокумент2 страницыLab Manual Animal Systematic II 2017 - Activity IVio Indah BudiartiОценок пока нет
- 2Документ78 страниц2api-3744136Оценок пока нет
- Multiple Pregnancy NOR PosterДокумент1 страницаMultiple Pregnancy NOR PosterbigbossОценок пока нет
- PCOSДокумент3 страницыPCOSpravallikakvОценок пока нет
- Effects of Early Pregnancy To StudentsДокумент30 страницEffects of Early Pregnancy To Studentsrejenkaye_0871% (7)
- Who PCPNC PDFДокумент179 страницWho PCPNC PDFTiffany Joyce MarcellanaОценок пока нет
- Quality of Postnatal Care ServicesДокумент10 страницQuality of Postnatal Care Servicessaleha sultanaОценок пока нет
- Endometriosis GuidelineДокумент44 страницыEndometriosis GuidelineHen DriОценок пока нет
- Incect AnatomiaДокумент14 страницIncect AnatomiaKrisztina Margit HorváthОценок пока нет
- Selection of Foundation Stocks and Breeding MethodsДокумент7 страницSelection of Foundation Stocks and Breeding Methodsdelacruz.nonaОценок пока нет
- Drosophila MelanogasterДокумент13 страницDrosophila MelanogasterDavid MorganОценок пока нет
- Anabolic SteroidsДокумент11 страницAnabolic Steroidsgramatolina100% (1)
- Human CloningДокумент2 страницыHuman CloningYhan SubaОценок пока нет
- Menstrual Disorder and Abnormal BleedingДокумент9 страницMenstrual Disorder and Abnormal Bleedingdr_asalehОценок пока нет
- Clinical Guideline: South Australian Perinatal Practice Guidelines - Cord Presentation and ProlapseДокумент9 страницClinical Guideline: South Australian Perinatal Practice Guidelines - Cord Presentation and ProlapseMelissa Aina Mohd YusofОценок пока нет