Вам также может понравиться
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaДокумент36 страницATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Hepatitis AutoimunДокумент32 страницыHepatitis AutoimunRofi IrmanОценок пока нет
- Drug Induced Hepatitis With Anti-Tubercular Chemotherapy: Challenges and Difficulties in TreatmentДокумент5 страницDrug Induced Hepatitis With Anti-Tubercular Chemotherapy: Challenges and Difficulties in Treatmentmufqifitra160491Оценок пока нет
- Autoimmune HepatitisДокумент3 страницыAutoimmune HepatitisMohammed FaragОценок пока нет
- Autoimmune HepatitisДокумент34 страницыAutoimmune HepatitisFUTURE DOCTORОценок пока нет
- DiliДокумент25 страницDiliSenarathKuleeshaKodisingheОценок пока нет
- Speaker-Arindam Pande Chairperson - Prof. B K Dey Prof. S B GangulyДокумент66 страницSpeaker-Arindam Pande Chairperson - Prof. B K Dey Prof. S B GangulyhananОценок пока нет
- 24 OctДокумент38 страниц24 OctVenkatesh JaiswalОценок пока нет
- Hipertransaminasemia Com Marcadores Virales NegativosДокумент17 страницHipertransaminasemia Com Marcadores Virales NegativosJAvier Rodriguez-VeraОценок пока нет
- Chemical Pathology II HIV AIDSДокумент33 страницыChemical Pathology II HIV AIDSSimeon AdebisiОценок пока нет
- 6 Ashkin 062012Документ79 страниц6 Ashkin 062012Anonymous QPXAgjBwОценок пока нет
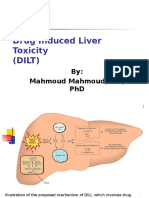
- Drug Induced Liver Toxicity-FinalДокумент39 страницDrug Induced Liver Toxicity-FinalAjeng SekariniОценок пока нет
- Att Hepatitis IndiaДокумент8 страницAtt Hepatitis IndiaDjabhi SpinzzОценок пока нет
- Autoimmune Hepatitis: Ermias Kacha (MD)Документ39 страницAutoimmune Hepatitis: Ermias Kacha (MD)kachapaxxОценок пока нет
- Drug Induced Liver Diseases (DILD) : M. DeepalakshmiДокумент22 страницыDrug Induced Liver Diseases (DILD) : M. DeepalakshmicrissОценок пока нет
- Evaluation of Abnormal Liver Function Tests: DR Chris Hovell Consultant Gastroenterologist Dorset County HospitalДокумент59 страницEvaluation of Abnormal Liver Function Tests: DR Chris Hovell Consultant Gastroenterologist Dorset County HospitalSaad MotawéaОценок пока нет
- Drug Induced Iliver InjuryДокумент36 страницDrug Induced Iliver InjuryAnjanieОценок пока нет
- Acute Liver FailureДокумент28 страницAcute Liver FailureAravind VPОценок пока нет
- Journal Reading ATDILIДокумент23 страницыJournal Reading ATDILIRiyang Pradewa AdmawanОценок пока нет
- Non Viral HepatitisДокумент40 страницNon Viral Hepatitisostaz2000100% (1)
- Bookshelf NBK548889Документ18 страницBookshelf NBK548889Rizqan Fahlevvi AkbarОценок пока нет
- RajaniДокумент8 страницRajaniArnette Castro de GuzmanОценок пока нет
- Management of AntiTB Induced HepatitisДокумент6 страницManagement of AntiTB Induced Hepatitisadilah fazliОценок пока нет
- Complementary and Alternative Medical Lab Testing Part 8: UrologyОт EverandComplementary and Alternative Medical Lab Testing Part 8: UrologyРейтинг: 3 из 5 звезд3/5 (1)
- Hepatotoxicity From Biologics?: Ross Pierce, M.D. Division of Hematology, Obrr/Cber/FdaДокумент16 страницHepatotoxicity From Biologics?: Ross Pierce, M.D. Division of Hematology, Obrr/Cber/Fdansk79in@gmail.comОценок пока нет
- Hepatotoxicity Related To Anti-Tuberculosis Drugs: Mechanisms and ManagementДокумент13 страницHepatotoxicity Related To Anti-Tuberculosis Drugs: Mechanisms and ManagementkhacthuanprovipОценок пока нет
- Valproic Acid Induced Acute Liver Injury Resulting in Hepatic Encephalopathy - A Case Report and Literature Review - PMCДокумент7 страницValproic Acid Induced Acute Liver Injury Resulting in Hepatic Encephalopathy - A Case Report and Literature Review - PMCdoodyОценок пока нет
- Antituberculosis: Drug-Induced Hepatiti: Risk Factors PR Ntion and ManagementДокумент7 страницAntituberculosis: Drug-Induced Hepatiti: Risk Factors PR Ntion and Managementmufqifitra160491Оценок пока нет
- Falla HepaticaДокумент24 страницыFalla HepaticaCbrera ValentinaОценок пока нет
- Meyer 2010Документ24 страницыMeyer 2010deltanueveОценок пока нет
- Drug Induced LiverДокумент8 страницDrug Induced LiverDita IndahОценок пока нет
- Case ReportДокумент5 страницCase ReportAlfi YatunОценок пока нет
- International Reports: Incidence of Hepatotoxicity Due To Antitubercular Medicines and Assessment of Risk FactorsДокумент6 страницInternational Reports: Incidence of Hepatotoxicity Due To Antitubercular Medicines and Assessment of Risk FactorsWelki VernandoОценок пока нет
- Acute HepatitisДокумент36 страницAcute HepatitisMuhammad BilalОценок пока нет
- Komplit Kasus Ingris ES Edit 22 Agusts 2013Документ48 страницKomplit Kasus Ingris ES Edit 22 Agusts 2013YhooogaОценок пока нет
- Abnormal LTs 2014Документ63 страницыAbnormal LTs 2014Robert G. Gish, MDОценок пока нет
- Lesson 1A - What Is DILIДокумент9 страницLesson 1A - What Is DILIAbin PОценок пока нет
- Interpretación Del Perfil HepáticoДокумент10 страницInterpretación Del Perfil HepáticoEdwin AlvarezОценок пока нет
- MJVH - Volume 4.2 - Issue 2 - Pages 53-55Документ3 страницыMJVH - Volume 4.2 - Issue 2 - Pages 53-55Indra YaniОценок пока нет
- Ibrt 06 I 4 P 232Документ2 страницыIbrt 06 I 4 P 232Aditia Nata KusumaОценок пока нет
- HepatitisДокумент5 страницHepatitisnurhasanah2112Оценок пока нет
- TB Drug Induced Liver Injury 27aug2013Документ39 страницTB Drug Induced Liver Injury 27aug2013Edi Uchiha SutarmantoОценок пока нет
- Acute Liver FailureДокумент39 страницAcute Liver FailurepascalmugodoОценок пока нет
- Phenelzine - Liver ToxicityДокумент8 страницPhenelzine - Liver Toxicitydo leeОценок пока нет
- Medical Diseases Complicating Pregnancy: by The Name of AllahДокумент45 страницMedical Diseases Complicating Pregnancy: by The Name of Allah'محمد علي' محمد لافيОценок пока нет
- 2005 Herbal Hepatotoxicity. Acute Hepatitis Caused by A Noni Preparation. EJGHДокумент3 страницы2005 Herbal Hepatotoxicity. Acute Hepatitis Caused by A Noni Preparation. EJGHJoseloОценок пока нет
- 121 - Perlemakan Hati 1Документ42 страницы121 - Perlemakan Hati 1Rulianis ApriantiОценок пока нет
- Acute Liver FailureДокумент78 страницAcute Liver FailurePankaj IngleОценок пока нет
- Document 2Документ2 страницыDocument 2velsyasukriaОценок пока нет
- Agents For Influenza A and Respiratory VirusesДокумент10 страницAgents For Influenza A and Respiratory VirusesTrixia RodulfaОценок пока нет
- Drug-Induced Liver Disease.Документ16 страницDrug-Induced Liver Disease.Dr. Ammar Khalil100% (1)
- HyperthyroidДокумент7 страницHyperthyroidHaerun Nisa SiregarОценок пока нет
- Chronic Liver DiseaseДокумент75 страницChronic Liver DiseasebitspurОценок пока нет
- He Pat OlogyДокумент20 страницHe Pat OlogytaosifОценок пока нет
- Overview of Autoimmune Hepatitis - UpToDateДокумент33 страницыOverview of Autoimmune Hepatitis - UpToDatebagir_dm10Оценок пока нет
- Tuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghДокумент3 страницыTuberculosis in Liver Cirrhosis: Rajesh Upadhyay, Aesha SinghAnastasia Lilian SuryajayaОценок пока нет
- Acut Hepatic FailureДокумент11 страницAcut Hepatic FailureDennis CobbОценок пока нет
- Clinicalmanifestationsand Treatmentofdrug-Induced HepatotoxicityДокумент9 страницClinicalmanifestationsand Treatmentofdrug-Induced HepatotoxicityChâu Khắc ToànОценок пока нет
- Perlemakan HatiДокумент42 страницыPerlemakan HatiSarital BoronОценок пока нет
- Complementary and Alternative Medical Lab Testing Part 14: ImmunologyОт EverandComplementary and Alternative Medical Lab Testing Part 14: ImmunologyОценок пока нет
- Attendance (20 - 06)Документ1 страницаAttendance (20 - 06)FahadKamalОценок пока нет
- Attendance - AДокумент1 страницаAttendance - AFahadKamalОценок пока нет
- Attendance (22 - 06)Документ1 страницаAttendance (22 - 06)FahadKamalОценок пока нет
- Office of The phase-IV Co-Ordinator Popular Medical College, DhakaДокумент1 страницаOffice of The phase-IV Co-Ordinator Popular Medical College, DhakaFahadKamalОценок пока нет
- Long Cases in Clinical Medicine PDFДокумент844 страницыLong Cases in Clinical Medicine PDFFahadKamal100% (4)
- Management of Tuberculosis in Special Situations: Prof. Dr. Zafar Hussain IqbalДокумент27 страницManagement of Tuberculosis in Special Situations: Prof. Dr. Zafar Hussain IqbalFahadKamalОценок пока нет
- Brain Health Dramatically Improved by Intake of OmegaДокумент18 страницBrain Health Dramatically Improved by Intake of OmegaAbdul Rasheed100% (1)
- Relationship of Self-Regulation, Stress, and Life Satisfaction Among Middle School Students of Ekamai International School, Bangkok, ThailandДокумент27 страницRelationship of Self-Regulation, Stress, and Life Satisfaction Among Middle School Students of Ekamai International School, Bangkok, ThailandFrederick Edward FabellaОценок пока нет
- What Are The Psychological Effects of Disaster Work On An Emergency Manager?Документ13 страницWhat Are The Psychological Effects of Disaster Work On An Emergency Manager?api-525064413Оценок пока нет
- Swine Infectious Gastrointestinal DiseasesДокумент6 страницSwine Infectious Gastrointestinal DiseasesnessimmounirОценок пока нет
- топик a visit to a dentistДокумент2 страницытопик a visit to a dentistEyeless DanteJackОценок пока нет
- What Is PovertyДокумент13 страницWhat Is PovertyNurul FaizaahОценок пока нет
- Russian Current Shiva Sarari 1Документ25 страницRussian Current Shiva Sarari 1Sharma MukeshОценок пока нет
- Aurobindo Pharma Receives USFDA Approval For Norethindrone Acetate Tablets (Company Update)Документ1 страницаAurobindo Pharma Receives USFDA Approval For Norethindrone Acetate Tablets (Company Update)Shyam SunderОценок пока нет
- Internal Medicine NBME Form 3 ExplanationsДокумент11 страницInternal Medicine NBME Form 3 ExplanationssasghfdgОценок пока нет
- What Are Drug ClassificationsДокумент5 страницWhat Are Drug ClassificationsCarl LewisОценок пока нет
- Management of Intravascular Devices To Prevent Infection: LinicalДокумент5 страницManagement of Intravascular Devices To Prevent Infection: LinicalCristianMedranoVargasОценок пока нет
- RPH 2Документ3 страницыRPH 2AYEN AROBINTOОценок пока нет
- Disaster Management Continuum Pre-DisasterДокумент2 страницыDisaster Management Continuum Pre-DisasterPearl JuntillaОценок пока нет
- Live Well With Asthma 2019Документ21 страницаLive Well With Asthma 2019GrigoreОценок пока нет
- NCP Hyperbilirubinemia Staff NursingДокумент3 страницыNCP Hyperbilirubinemia Staff NursingVerajoy DaanОценок пока нет
- Australian Indigenous People - EditedДокумент8 страницAustralian Indigenous People - EditedApril CliffordОценок пока нет
- Prescription Pain MedicationДокумент9 страницPrescription Pain Medicationapi-409112773Оценок пока нет
- A Risk and ResilienceДокумент20 страницA Risk and ResilienceFlaviu Alexandru MoraruОценок пока нет
- Pharmacoeconomics: Dr. Salim Sheikh Dept. of Pharmacology, VMMC & Safdarjung HospitalДокумент80 страницPharmacoeconomics: Dr. Salim Sheikh Dept. of Pharmacology, VMMC & Safdarjung HospitalSima JabbariОценок пока нет
- Psition Paper - Salupare - Ervin - DДокумент2 страницыPsition Paper - Salupare - Ervin - DErvin SalupareОценок пока нет
- Case Study OrthopedicДокумент15 страницCase Study Orthopedicjoyevangelista100% (3)
- MCQ of NeurologyДокумент45 страницMCQ of Neurologyeffe26100% (7)
- Chris Korhonian Korhonian 1Документ6 страницChris Korhonian Korhonian 1api-535175658Оценок пока нет
- Adult Obesity ResearchДокумент19 страницAdult Obesity Researchchoraz100% (1)
- Dental Negligence in Clinical PracticeДокумент18 страницDental Negligence in Clinical PracticeLutfun NessaОценок пока нет
- Importance of Outdoor Play Literature ReviewДокумент8 страницImportance of Outdoor Play Literature Reviewafmzadevfeeeat100% (1)
- 5 Elements of Abdominal DiagnosisДокумент14 страниц5 Elements of Abdominal Diagnosiscelliastt100% (4)
- Follow UpДокумент36 страницFollow UpAlegria03Оценок пока нет
- Policy Brief:: South Africa and The Hiv/Aids Question: Will The Government Ever Find A Solution?Документ13 страницPolicy Brief:: South Africa and The Hiv/Aids Question: Will The Government Ever Find A Solution?Ipeleng BosilongОценок пока нет
- Running Head: Mass Incarceration and Politics 1Документ16 страницRunning Head: Mass Incarceration and Politics 1kimoda freelancerОценок пока нет