Вам также может понравиться
- Endocrine NursingДокумент16 страницEndocrine NursingFreeNursingNotes100% (18)
- Human Body Systems OverviewДокумент6 страницHuman Body Systems OverviewEgi Rivas100% (1)
- Informative SpeechДокумент3 страницыInformative Speechapi-34039500550% (2)
- Unit 3 Study GuideДокумент10 страницUnit 3 Study GuideangieswensonОценок пока нет
- Exfoliative CytologyДокумент1 страницаExfoliative CytologyNathaniel SimОценок пока нет
- Boys Puberty ChangesДокумент6 страницBoys Puberty ChangesNata LiaОценок пока нет
- Corticosteroids 2 of 2Документ33 страницыCorticosteroids 2 of 2VLDsОценок пока нет
- Impact of Genetically-Modified Organisms On The EnvironmentДокумент23 страницыImpact of Genetically-Modified Organisms On The Environmentмарина нещеретОценок пока нет
- Venipuncture A Process of Collecting or "Drawing" Blood From A Vein ofДокумент38 страницVenipuncture A Process of Collecting or "Drawing" Blood From A Vein ofVera June RañesesОценок пока нет
- Lab Report Assistant Endocrine SystemДокумент7 страницLab Report Assistant Endocrine SystemJohn Louis AguilaОценок пока нет
- Lesson 5Документ8 страницLesson 5Iris John Lentija DoncilloОценок пока нет
- Nutrition across the Lifespan: Pregnancy, Lactation and InfancyДокумент9 страницNutrition across the Lifespan: Pregnancy, Lactation and InfancyCorpus, Irene Zen P.Оценок пока нет
- ContraceptionДокумент9 страницContraceptionsarguss14100% (4)
- Global City and Global DemographyДокумент3 страницыGlobal City and Global DemographyDessaОценок пока нет
- Essay Project 2Документ6 страницEssay Project 2api-535694195Оценок пока нет
- Fertilization-Early Embryo Dev'tДокумент38 страницFertilization-Early Embryo Dev'tMae T OlivaОценок пока нет
- Cell Cycle Coloring KeyДокумент8 страницCell Cycle Coloring KeyKen Brian Edward MaliaoОценок пока нет
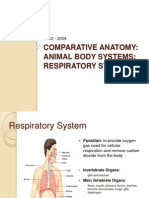
- Respiratory SystemДокумент13 страницRespiratory SystemRifai Alfarabi100% (1)
- Unit 3 - Dynamic Equilibrium Section 6-Immune System: Biology 2201Документ23 страницыUnit 3 - Dynamic Equilibrium Section 6-Immune System: Biology 2201Vivek Gupta100% (2)
- Endocrine SystemДокумент58 страницEndocrine SystemRochelle Jade Docejo IIОценок пока нет
- Salmonella Reflection PDFДокумент2 страницыSalmonella Reflection PDFcОценок пока нет
- Human Reproductive System WebsiteДокумент46 страницHuman Reproductive System Websiteapi-258400031Оценок пока нет
- Pig Heart Dissection Lab - Final PDFДокумент15 страницPig Heart Dissection Lab - Final PDFapi-1127245210% (1)
- Reproductive Health Bill in The PhilippinesДокумент4 страницыReproductive Health Bill in The PhilippinesJhazzryll Catanes MocayОценок пока нет
- Lipid MetabolismДокумент472 страницыLipid MetabolismPovoljanPrevodОценок пока нет
- Key Figures of the Intellectual RevolutionДокумент6 страницKey Figures of the Intellectual RevolutionJonathanОценок пока нет
- Org-Incentives-strategy-global Corp Banking at CitibankДокумент36 страницOrg-Incentives-strategy-global Corp Banking at CitibankShivanjali KambleОценок пока нет
- CC CheckДокумент105 страницCC CheckMarie LlanesОценок пока нет
- Water Soluble VitaminsДокумент6 страницWater Soluble VitaminsMabesОценок пока нет
- Abortion Group AssignmentДокумент26 страницAbortion Group AssignmentJr Ajayi BОценок пока нет
- Onion Dna IsolationДокумент4 страницыOnion Dna IsolationSmriti SmreetiОценок пока нет
- Compilation Medsurg PrelimsДокумент29 страницCompilation Medsurg PrelimsEunice CuñadaОценок пока нет
- 3rd Meeting.4. ROLE OF THE YOUTH ON THE DRUG PREVENTION. October 10, 2020Документ15 страниц3rd Meeting.4. ROLE OF THE YOUTH ON THE DRUG PREVENTION. October 10, 2020Wynona Balandra50% (2)
- Brief History of Key Men in BiologyДокумент17 страницBrief History of Key Men in BiologyCarlo AcebronОценок пока нет
- The Skeletal System ExplainedДокумент6 страницThe Skeletal System Explainedstar fireОценок пока нет
- Speech 4 Sex EducationДокумент12 страницSpeech 4 Sex EducationAdof Addar MudhoffarОценок пока нет
- Biochem FinalsДокумент14 страницBiochem FinalsMemeowwОценок пока нет
- Nutrition and MetabolismДокумент9 страницNutrition and MetabolismarunatejaОценок пока нет
- Biochemistry Quiz - Enzymes and Vitamins - Answer KeyДокумент8 страницBiochemistry Quiz - Enzymes and Vitamins - Answer KeyKennethОценок пока нет
- Ethics 2Документ19 страницEthics 2Roriel Hernandez BenamirОценок пока нет
- Chapter Ii: Biochemical Perspective in Gender and Sexuality Lesson 1: Anatomy and Physiology of ReproductionДокумент10 страницChapter Ii: Biochemical Perspective in Gender and Sexuality Lesson 1: Anatomy and Physiology of ReproductionDevin Jake Maylas FeoОценок пока нет
- Protein Digestion & AbsorptionДокумент23 страницыProtein Digestion & AbsorptionMaryОценок пока нет
- Responsible NetizenshipДокумент26 страницResponsible NetizenshipMArk Anthony ArtisОценок пока нет
- 11 Systems of The BodyДокумент11 страниц11 Systems of The BodyYamSomandarОценок пока нет
- The Sexual SelfДокумент18 страницThe Sexual SelfAngelo Dale Derramas OndilloОценок пока нет
- Male Reproductive SystemДокумент30 страницMale Reproductive SystemRaisashimi M.S.100% (1)
- VanPutte Seeleys Essentials 11e Chap07 PPT AccessibleДокумент109 страницVanPutte Seeleys Essentials 11e Chap07 PPT AccessibleYhel Trinidad50% (2)
- The Urinary System: Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical CollegeДокумент91 страницаThe Urinary System: Prepared by Patty Bostwick-Taylor, Florence-Darlington Technical CollegeNicole NipasОценок пока нет
- Module 12 - The Aspect of Gene TherapyДокумент4 страницыModule 12 - The Aspect of Gene TherapyMark Daniel DeTorres GolisaoОценок пока нет
- Host TypesДокумент14 страницHost TypesMayuri Vohra100% (1)
- Antibiotics: Classification and Mechanisms of Action With Emphasis On Molecular PerspectivesДокумент13 страницAntibiotics: Classification and Mechanisms of Action With Emphasis On Molecular PerspectivesNishant ShresthaОценок пока нет
- Pharma Trans Le1Документ60 страницPharma Trans Le1Kunal TribhuvanОценок пока нет
- Philippine Health Care and The Philippine Health Care Delivery SystemДокумент19 страницPhilippine Health Care and The Philippine Health Care Delivery SystemJennifer Ledesma-PidoОценок пока нет
- Comparing the Tissue Organization of Monocot and Dicot RootsДокумент9 страницComparing the Tissue Organization of Monocot and Dicot RootsmasorОценок пока нет
- Marc Johanna L. Villacora Activity 2.1 Citizenship TrainingДокумент6 страницMarc Johanna L. Villacora Activity 2.1 Citizenship TrainingDhision VillacoraОценок пока нет
- MenstruationДокумент16 страницMenstruationAnnsha VeimernОценок пока нет
- PDFДокумент5 страницPDFZyan MОценок пока нет
- Overview of Health Informatics: Lesson 4Документ8 страницOverview of Health Informatics: Lesson 4Jennifer Ledesma-PidoОценок пока нет
- N-Week 9 The ConstitutionsДокумент9 страницN-Week 9 The ConstitutionsJayann AbilaОценок пока нет
- The Philippines in Ancient TimesДокумент33 страницыThe Philippines in Ancient TimesKen StarОценок пока нет
- 09 Exocytosis and EndocytosisДокумент6 страниц09 Exocytosis and Endocytosisdrhendyjunior100% (1)
- Endocrine PhysiologyДокумент98 страницEndocrine PhysiologyMohan GuptaОценок пока нет
- Starling Forces Across The Capillary WallДокумент1 страницаStarling Forces Across The Capillary WallphyMedza AppОценок пока нет
- Effects of Adding Solutes To The ECF On Compartment SizeДокумент1 страницаEffects of Adding Solutes To The ECF On Compartment SizephyMedza AppОценок пока нет
- Body Fluid CompartmentДокумент1 страницаBody Fluid CompartmentphyMedza AppОценок пока нет
- Membrane ProteinsДокумент1 страницаMembrane ProteinsphyMedza AppОценок пока нет
- Cell MembraneДокумент100 страницCell MembranephyMedza AppОценок пока нет
- Cellmembrane and Transport Mechanism PDFДокумент78 страницCellmembrane and Transport Mechanism PDFphyMedza AppОценок пока нет
- Introduction To Physiology and Concept of HomeostasisДокумент36 страницIntroduction To Physiology and Concept of HomeostasisphyMedza AppОценок пока нет
- Disease of The Endocrine Gland Hyposecretion & HypersecretionДокумент4 страницыDisease of The Endocrine Gland Hyposecretion & HypersecretionNurul HusnaОценок пока нет
- Disorders of Water and Sodium BalanceДокумент21 страницаDisorders of Water and Sodium BalanceStanОценок пока нет
- Introduction To Pituitary GlandДокумент7 страницIntroduction To Pituitary GlandRoman KhanОценок пока нет
- ICU Reading on Pathophysiology and Management of Posttraumatic Diabetes InsipidusДокумент24 страницыICU Reading on Pathophysiology and Management of Posttraumatic Diabetes Insipidus駱品全Оценок пока нет
- Fluid and Electrolyte ImbalanceДокумент27 страницFluid and Electrolyte ImbalanceSimmi Sidhu100% (1)
- 2J Coordination: Time: 1 Hour 5 Minutes Total Marks Available: 65 Total Marks AchievedДокумент26 страниц2J Coordination: Time: 1 Hour 5 Minutes Total Marks Available: 65 Total Marks AchievedRabia RafiqueОценок пока нет
- Investigations in Psychiatry Guide Medical DiagnosesДокумент59 страницInvestigations in Psychiatry Guide Medical Diagnoseskiran mahal100% (1)
- OsmoregulationДокумент6 страницOsmoregulationNIRBHAY_BARDIYAОценок пока нет
- ELECTROLYTES Na KДокумент8 страницELECTROLYTES Na KMicael MendozaОценок пока нет
- Endocrine System - MedДокумент124 страницыEndocrine System - Medrediet shimekachОценок пока нет
- Surgery Quiz Topics 1 5Документ48 страницSurgery Quiz Topics 1 5Hello AngelОценок пока нет
- Sample Ch05Документ53 страницыSample Ch05mb_13_throwawayОценок пока нет
- Endocrine Disorders-1Документ52 страницыEndocrine Disorders-1Nathaniel Mbiu TimОценок пока нет
- Water Regulation - Indd - OsmosisДокумент7 страницWater Regulation - Indd - OsmosisRishi Raj NRОценок пока нет
- Hypothalamus and Pituitary Gland FunctionsДокумент48 страницHypothalamus and Pituitary Gland FunctionsMohsin AbbasОценок пока нет
- Hypothalamus - Anterior Pituitary and Their HormonesДокумент138 страницHypothalamus - Anterior Pituitary and Their HormonesML Rodriguez100% (1)
- Sodium, Water and Potassium: Michael D. PenneyДокумент39 страницSodium, Water and Potassium: Michael D. PenneyChristianus LeonardОценок пока нет
- HAPL4 - HUMAN ANATOMY and PHYSIOLOGY - MODULE 4 & 5Документ47 страницHAPL4 - HUMAN ANATOMY and PHYSIOLOGY - MODULE 4 & 5welpОценок пока нет
- Endocrine System Chapter SummaryДокумент6 страницEndocrine System Chapter SummaryShiny ChenОценок пока нет
- Pharmacology Diuretics For BPT StudentsДокумент16 страницPharmacology Diuretics For BPT StudentsDr.U.P.Rathnakar.MD.DIH.PGDHM100% (1)
- Dr. Bambang Tridjaja - Hyponatremia Endocrin ApproachДокумент42 страницыDr. Bambang Tridjaja - Hyponatremia Endocrin ApproachayushintamahaputriОценок пока нет
- Neurocritical Care PDFДокумент40 страницNeurocritical Care PDFAzima AbdelrhamanОценок пока нет
- EMRA Sepsis CardДокумент4 страницыEMRA Sepsis Cardsgod34100% (1)
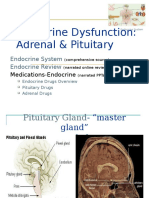
- Endocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewДокумент102 страницыEndocrine Dysfunction: Adrenal & Pituitary: Endocrine System Endocrine ReviewCalimlim KimОценок пока нет
- Review in AUBFДокумент37 страницReview in AUBFMichelle T. MabasaОценок пока нет
- Endocrine ConditionsДокумент5 страницEndocrine ConditionsGlen DizonОценок пока нет
- Mangement 2 PDFДокумент165 страницMangement 2 PDFjanveeОценок пока нет
- Endocrine ResonanceДокумент51 страницаEndocrine ResonanceEkta ManglaniОценок пока нет