Вам также может понравиться
- Natural Abortion MethodsДокумент10 страницNatural Abortion MethodsSury Ganesh100% (1)
- Dietary Guide for Maternal NutritionДокумент6 страницDietary Guide for Maternal NutritionSandra Saenz de TejadaОценок пока нет
- Nutrition in PregnancyДокумент32 страницыNutrition in PregnancyherwindakОценок пока нет
- Hospital-Based Triage of Obstetric Patients ACOGДокумент4 страницыHospital-Based Triage of Obstetric Patients ACOGponekОценок пока нет
- Nutrition in PregnancyДокумент5 страницNutrition in PregnancyCatalin SimionОценок пока нет
- Lesson-2 Heredity, Prenatal Development, and Birth PDFДокумент64 страницыLesson-2 Heredity, Prenatal Development, and Birth PDFchat gazaОценок пока нет
- Maternal NutritionДокумент16 страницMaternal NutritionAbdur RehmanОценок пока нет
- Wellness PDFДокумент295 страницWellness PDFsimianchanОценок пока нет
- Aquino V Delizo (Digest)Документ2 страницыAquino V Delizo (Digest)Yvette Morales100% (1)
- Nutrition Guideline PregnancyДокумент27 страницNutrition Guideline PregnancyMuhammad FauziОценок пока нет
- Nutrition Throughout The Life CycleДокумент87 страницNutrition Throughout The Life Cyclealsuwaidi5Оценок пока нет
- QSGTL Tank Jacking & Bottom Replacement ProjectДокумент28 страницQSGTL Tank Jacking & Bottom Replacement ProjectShrikant Moje100% (1)
- Dr. Etisa - Nutrition in PregnancyДокумент71 страницаDr. Etisa - Nutrition in Pregnancynur chasanahОценок пока нет
- Ob PamphletДокумент2 страницыOb Pamphletapi-305460281100% (3)
- Sss & Gsis LawДокумент57 страницSss & Gsis Lawjenricke2003100% (3)
- Nutrition and Diet Therapy Pregnancy Lactation Infancy Childhood School AgeДокумент176 страницNutrition and Diet Therapy Pregnancy Lactation Infancy Childhood School AgeZeheriahОценок пока нет
- Duplex MetrodeДокумент16 страницDuplex MetrodeShrikant MojeОценок пока нет
- Manual Also 2017 (1) (001-160)Документ160 страницManual Also 2017 (1) (001-160)Diana Calderon SolisОценок пока нет
- Updated Resume CeciliaДокумент3 страницыUpdated Resume CeciliaRommel Jhon RiveraОценок пока нет
- Postnatal Depletion - GoopДокумент7 страницPostnatal Depletion - GoopLaura100% (1)
- API RP 571 Test QuestionsДокумент22 страницыAPI RP 571 Test QuestionsShrikant Moje100% (1)
- Manufacturing ProcessesДокумент477 страницManufacturing ProcessesVinod89% (19)
- Manufacturing ProcessesДокумент477 страницManufacturing ProcessesVinod89% (19)
- Vaccinations in PregnancyДокумент137 страницVaccinations in PregnancyAmine YounisОценок пока нет
- Nutrition Through The Lifespan and Diet and Disease BackupДокумент67 страницNutrition Through The Lifespan and Diet and Disease BackupJessica SnowОценок пока нет
- General Damage Mechanisms and Corrosion Failure ModesДокумент6 страницGeneral Damage Mechanisms and Corrosion Failure ModesShrikant Moje100% (1)
- General Damage Mechanisms and Corrosion Failure ModesДокумент6 страницGeneral Damage Mechanisms and Corrosion Failure ModesShrikant Moje100% (1)
- General Damage Mechanisms and Corrosion Failure ModesДокумент6 страницGeneral Damage Mechanisms and Corrosion Failure ModesShrikant Moje100% (1)
- Interpass Temperature WeldingДокумент2 страницыInterpass Temperature Weldinghareesh13hОценок пока нет
- Gas Shielded Flux Cored Arc Welding (FCAW) GuideДокумент19 страницGas Shielded Flux Cored Arc Welding (FCAW) GuideSanthosh Kumar100% (1)
- Gas Shielded Flux Cored Arc Welding (FCAW) GuideДокумент19 страницGas Shielded Flux Cored Arc Welding (FCAW) GuideSanthosh Kumar100% (1)
- Electrode PDFДокумент32 страницыElectrode PDFShrikant MojeОценок пока нет
- Maternal Child Tracking Sysem PDFДокумент9 страницMaternal Child Tracking Sysem PDFMegha MalhiОценок пока нет
- Nutrition in PregnancyДокумент16 страницNutrition in PregnancynkhomaslaterОценок пока нет
- Nutrition Care During Pregnancy and LactationДокумент10 страницNutrition Care During Pregnancy and LactationSophy ChelotiОценок пока нет
- Unit 1 Maternal Nutrition, Educational PlatformДокумент76 страницUnit 1 Maternal Nutrition, Educational Platformzia ullahОценок пока нет
- Jurnal PDFДокумент5 страницJurnal PDFWaica PratiwiОценок пока нет
- 3 Nutrition, Pain Management During LaborДокумент52 страницы3 Nutrition, Pain Management During LaborJoshua Isiah S. LumapasОценок пока нет
- Maternal Lec Semi-FinalsДокумент433 страницыMaternal Lec Semi-FinalsTrishaОценок пока нет
- Guidelines in Weight Gain and PregnancyДокумент20 страницGuidelines in Weight Gain and PregnancyAmon RAОценок пока нет
- How Being Underweight During Pregnancy Can Affect You and Your BabyДокумент7 страницHow Being Underweight During Pregnancy Can Affect You and Your BabyRhaiza RebustilloОценок пока нет
- Nutrition in pregnancy essentialsДокумент51 страницаNutrition in pregnancy essentialsEnik guntyastutikОценок пока нет
- Normal Diagnostic and Laboratory Findings/ Nutritional Health of Pregnant WomenДокумент8 страницNormal Diagnostic and Laboratory Findings/ Nutritional Health of Pregnant WomenArianna Jasmine MabungaОценок пока нет
- Literature Review On Nutrition During PregnancyДокумент4 страницыLiterature Review On Nutrition During Pregnancyafdtwtdsa100% (1)
- Unit 22Документ9 страницUnit 222begeniusОценок пока нет
- Energy NeedsДокумент2 страницыEnergy NeedsXoisagesОценок пока нет
- Module 6nДокумент19 страницModule 6nMAZIMA FRANKОценок пока нет
- NTL Pregnancy and LactationДокумент50 страницNTL Pregnancy and Lactationkiamadine.deruedaОценок пока нет
- Pregnancy: Nutrition And Supplements For Expecting Mothers: Learn Everything You Need To Know To Optimally Nourish Yourself And Your BabyОт EverandPregnancy: Nutrition And Supplements For Expecting Mothers: Learn Everything You Need To Know To Optimally Nourish Yourself And Your BabyОценок пока нет
- Eating Well With Baby Belly: Healthy Eating While Pregnant (Pregnancy Nutrition Guide)От EverandEating Well With Baby Belly: Healthy Eating While Pregnant (Pregnancy Nutrition Guide)Оценок пока нет
- 发表 修正Документ2 страницы发表 修正郑心洁Оценок пока нет
- Nutrition & Healthy DietRRДокумент55 страницNutrition & Healthy DietRRVonderОценок пока нет
- Obesity and PregnancyДокумент4 страницыObesity and PregnancyRL FlacamaОценок пока нет
- IgwgДокумент26 страницIgwgapi-285904462Оценок пока нет
- Maternal Nutrition During Pregnancy and LactationДокумент11 страницMaternal Nutrition During Pregnancy and Lactationwinda sari wahyuniОценок пока нет
- Pakistan Dietary Guidline For Beeter NutritionДокумент21 страницаPakistan Dietary Guidline For Beeter NutritionNauman ShahzadОценок пока нет
- Tugas WindaДокумент11 страницTugas Windawinda sari wahyuniОценок пока нет
- Prevent Malnutrition in SeniorsДокумент3 страницыPrevent Malnutrition in SeniorsLegendXОценок пока нет
- Week 5: Nutrition Across The Lifespan (Pregnancy, Infacy, Toddler and Pre-SchoolДокумент12 страницWeek 5: Nutrition Across The Lifespan (Pregnancy, Infacy, Toddler and Pre-SchoolABEGAIL BALLORANОценок пока нет
- Research Paper On Nutrition in PregnancyДокумент5 страницResearch Paper On Nutrition in Pregnancyfys5ehgs100% (1)
- Maternal Nutrition EssentialsДокумент19 страницMaternal Nutrition EssentialsfarhanaОценок пока нет
- Midterms: NCM 105: Nutrition and Diet TherapyДокумент32 страницыMidterms: NCM 105: Nutrition and Diet TherapyJohn Ford VisoriaОценок пока нет
- Applied Nutrition Unit 01-1Документ36 страницApplied Nutrition Unit 01-1Hira KhanОценок пока нет
- Maternal Nutritional AssessmentДокумент7 страницMaternal Nutritional AssessmentchinchuОценок пока нет
- Week 2Документ56 страницWeek 2Wong ChocolateОценок пока нет
- Nutrition Essentials and the Importance of Good NutritionДокумент7 страницNutrition Essentials and the Importance of Good NutritionMira AurumtinОценок пока нет
- Magazine Article For Expecting MomsДокумент2 страницыMagazine Article For Expecting Momsapi-295221163Оценок пока нет
- Background of The Study: Sleep, Nausea and Vomiting Were Shown To Have Contribution To Antenatal Life QualityДокумент12 страницBackground of The Study: Sleep, Nausea and Vomiting Were Shown To Have Contribution To Antenatal Life QualityLizette Leah ChingОценок пока нет
- Nutritional Requirements Throughout The Lifecycle: Nutrition, The Human Life Span, or The MaximumДокумент33 страницыNutritional Requirements Throughout The Lifecycle: Nutrition, The Human Life Span, or The MaximumKent Adrian UnatoОценок пока нет
- Nutrition-GSCI1045 Lecture - Week 12Документ16 страницNutrition-GSCI1045 Lecture - Week 12Nicholas ObasiОценок пока нет
- Introd. To NutritionДокумент11 страницIntrod. To NutritionBenjamin KipandaОценок пока нет
- Knowledge and attitude of primigravida mothers regarding antenatal dietДокумент6 страницKnowledge and attitude of primigravida mothers regarding antenatal dietNeha RanaОценок пока нет
- Benefits of Breastfeeding For Mothers - Nutr 251 Honors AssignmentДокумент10 страницBenefits of Breastfeeding For Mothers - Nutr 251 Honors Assignmentapi-642953552Оценок пока нет
- Nutrition Final NotesДокумент32 страницыNutrition Final NotesCyrille Aira AndresaОценок пока нет
- Nutrition: Lamesginew MДокумент123 страницыNutrition: Lamesginew MWondimu EliasОценок пока нет
- Pregnancy Weight GainДокумент9 страницPregnancy Weight GainKevin MulyaОценок пока нет
- Brestfeeding Defense ObesityДокумент4 страницыBrestfeeding Defense ObesityChristine Notoningtiyas SantosoОценок пока нет
- Module 9 Pregnancy UpdatedДокумент4 страницыModule 9 Pregnancy UpdatedMARK JEFTE BRIONESОценок пока нет
- PDF Nutrition CM 1 CU 5 LEC WEEK 5Документ8 страницPDF Nutrition CM 1 CU 5 LEC WEEK 5gabbyОценок пока нет
- Obesity GuidelinesДокумент5 страницObesity GuidelinesKhalid BallaОценок пока нет
- ObesityДокумент35 страницObesitysohilaw210Оценок пока нет
- ICP™ Application Submission: User Guide For API 571, 577 and 580 ApplicantsДокумент23 страницыICP™ Application Submission: User Guide For API 571, 577 and 580 ApplicantsShrikant MojeОценок пока нет
- ICP™ Application Submission: User Guide For API 571, 577 and 580 ApplicantsДокумент23 страницыICP™ Application Submission: User Guide For API 571, 577 and 580 ApplicantsShrikant MojeОценок пока нет
- World Pipelines June 2007 - Integrity Management PDFДокумент6 страницWorld Pipelines June 2007 - Integrity Management PDFShrikant MojeОценок пока нет
- Api 571 HNДокумент1 страницаApi 571 HNShrikant MojeОценок пока нет
- ICP™ Application Submission: User Guide For API 571, 577 and 580 ApplicantsДокумент23 страницыICP™ Application Submission: User Guide For API 571, 577 and 580 ApplicantsShrikant MojeОценок пока нет
- Rajasthan Tour 9n10dДокумент2 страницыRajasthan Tour 9n10dShrikant MojeОценок пока нет
- World Pipelines June 2007 - Integrity ManagementДокумент55 страницWorld Pipelines June 2007 - Integrity ManagementShrikant MojeОценок пока нет
- Key Concepts 2 Heat InputДокумент4 страницыKey Concepts 2 Heat InputBama RamachandranОценок пока нет
- Fabrication Procedure FOR Evaporators: MFF Larsen & Toubro Limited Hazira Works, SuratДокумент51 страницаFabrication Procedure FOR Evaporators: MFF Larsen & Toubro Limited Hazira Works, SuratShrikant MojeОценок пока нет
- Key Concepts 2 Heat InputДокумент4 страницыKey Concepts 2 Heat InputBama RamachandranОценок пока нет
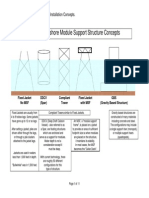
- 6.offshore ConceptsДокумент0 страниц6.offshore Conceptshaidar1992Оценок пока нет
- Piping DesignДокумент8 страницPiping Designswabha102Оценок пока нет
- Piping Surges PDFДокумент14 страницPiping Surges PDFiboОценок пока нет
- Key Concepts 2 Heat InputДокумент4 страницыKey Concepts 2 Heat InputBama RamachandranОценок пока нет
- Welding ProcessesДокумент78 страницWelding ProcessesShrikant MojeОценок пока нет
- Welding Consumanle SelectionДокумент85 страницWelding Consumanle SelectionShrikant MojeОценок пока нет
- ASME P-Numbers PDFДокумент2 страницыASME P-Numbers PDFShrikant Moje100% (1)
- Ductile Iron Pipe Methods of DesignДокумент22 страницыDuctile Iron Pipe Methods of DesignShrikant MojeОценок пока нет
- Bupa CarePro Consolidated 2017Документ30 страницBupa CarePro Consolidated 2017SSОценок пока нет
- Effect of Obesity On Assisted Reproductive TOG 2017Документ8 страницEffect of Obesity On Assisted Reproductive TOG 2017Muhammad Javed GabaОценок пока нет
- Abortion ReadingДокумент43 страницыAbortion ReadingJessica Lorenz PablicoОценок пока нет
- 9% Sodium Chloride Solution MSDSДокумент14 страниц9% Sodium Chloride Solution MSDSbidangОценок пока нет
- W1-L3-Human Development - Heredity and Environment200414060604044949Документ14 страницW1-L3-Human Development - Heredity and Environment200414060604044949Sachidananda AngomОценок пока нет
- Reproductive PharmacologyДокумент3 страницыReproductive PharmacologyNamarОценок пока нет
- Hideyuki Higuchi, M.D., Shunichi Takagi, M.D., Kan Zhang, M.D., Ikue Furui, M.D., Makoto Ozaki, M.DДокумент6 страницHideyuki Higuchi, M.D., Shunichi Takagi, M.D., Kan Zhang, M.D., Ikue Furui, M.D., Makoto Ozaki, M.DgoldenОценок пока нет
- Anchoring ScriptДокумент33 страницыAnchoring ScriptAparnaa SonaaОценок пока нет
- Integrating Family Planning and Antiretroviral Therapy-Service ModelДокумент138 страницIntegrating Family Planning and Antiretroviral Therapy-Service ModelApril Rose Airoso - AramburoОценок пока нет
- Nutritional Survey of Tea Garden WorkersДокумент11 страницNutritional Survey of Tea Garden Workerssupriyo92770% (1)
- Sifilis GestacionalДокумент15 страницSifilis Gestacionalrafael martinezОценок пока нет
- PMC Exam 2018Документ27 страницPMC Exam 2018Abed ElharazinОценок пока нет
- Environmental Risk Factors and Biomarkers For Autism Spectrum Disorder: An Umbrella Review of The EvidenceДокумент11 страницEnvironmental Risk Factors and Biomarkers For Autism Spectrum Disorder: An Umbrella Review of The EvidenceLaurenLuodiYuОценок пока нет
- Music, Arts, Physical Education, and Health (Mapeh) : Quarter 2 - Module 4Документ20 страницMusic, Arts, Physical Education, and Health (Mapeh) : Quarter 2 - Module 4KATRINA AL-LIANA CASUGAОценок пока нет
- Post DateДокумент40 страницPost DateDr-Firas Nayf Al-ThawabiaОценок пока нет
- Online Assignment 4Документ10 страницOnline Assignment 4Ab Staholic BoiiОценок пока нет
- Solution Manual For Applications and Investigations in Earth Science 7 e 7th EditionДокумент38 страницSolution Manual For Applications and Investigations in Earth Science 7 e 7th Editioncliverslaburnum46p3r7100% (10)
- Comprehensive Uworld ReviewДокумент190 страницComprehensive Uworld ReviewJoe JОценок пока нет
- Full-Term Fetus in Vertex PresentationДокумент1 страницаFull-Term Fetus in Vertex PresentationwhitecoatОценок пока нет