Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Test Help StatДокумент18 страницTest Help Statthenderson22603Оценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- ACCA P5 GTG Question Bank - 2011Документ180 страницACCA P5 GTG Question Bank - 2011raqifiluz86% (22)
- DTR For ReadingДокумент2 страницыDTR For ReadingTimosa TeyobОценок пока нет
- HYD CCU: TICKET - ConfirmedДокумент2 страницыHYD CCU: TICKET - ConfirmedRahul ValapadasuОценок пока нет
- Definition of Unit HydrographДокумент5 страницDefinition of Unit HydrographPankaj ChowdhuryОценок пока нет
- Talk - Data Quality FrameworkДокумент30 страницTalk - Data Quality FrameworkMatthew LawlerОценок пока нет
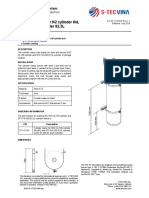
- Cylinder Clamp For N2 Cylinder 84L and FM-200 Cylinder 82.5LДокумент1 страницаCylinder Clamp For N2 Cylinder 84L and FM-200 Cylinder 82.5LNguyễn Minh ThiệuОценок пока нет
- GG&G 2012 CatДокумент111 страницGG&G 2012 Cattyrant88Оценок пока нет
- Food Safety and StandardsДокумент8 страницFood Safety and StandardsArifSheriffОценок пока нет
- Process and Inter-Process Systems For All Industries.: Cleaning Validation: An Overall PerspectiveДокумент7 страницProcess and Inter-Process Systems For All Industries.: Cleaning Validation: An Overall PerspectiveDesarrollo de Colecciones IVIC-BMRОценок пока нет
- Using Excel For Business AnalysisДокумент5 страницUsing Excel For Business Analysis11armiОценок пока нет
- Incident Log - TemplateДокумент10 страницIncident Log - TemplateRajaОценок пока нет
- 24th SFCON Parallel Sessions Schedule (For Souvenir Program)Документ1 страница24th SFCON Parallel Sessions Schedule (For Souvenir Program)genesistorres286Оценок пока нет
- Basic Principles of Immunology: Seminar OnДокумент43 страницыBasic Principles of Immunology: Seminar OnDr. Shiny KajalОценок пока нет
- DS - LWT300 - SF - A4 EN Rev BДокумент4 страницыDS - LWT300 - SF - A4 EN Rev BZts MksОценок пока нет
- Daftar Kalibrasi Peralatan MedisДокумент34 страницыDaftar Kalibrasi Peralatan Medisdiklat rssnОценок пока нет
- Emailing Prime - Brochure - DigitalДокумент32 страницыEmailing Prime - Brochure - DigitalCASA VALLIОценок пока нет
- Picasso OperatingInstructions Manual 211018 WEBДокумент27 страницPicasso OperatingInstructions Manual 211018 WEBBill McFarlandОценок пока нет
- CHAPTER 22-Audit Evidence EvaluationДокумент27 страницCHAPTER 22-Audit Evidence EvaluationIryne Kim PalatanОценок пока нет
- EC1002 Commentary 2022Документ32 страницыEC1002 Commentary 2022Xxx V1TaLОценок пока нет
- National School Building Inventory (NSBI) Encoding For SY 2021-2022Документ31 страницаNational School Building Inventory (NSBI) Encoding For SY 2021-2022Renato Rivera100% (1)
- Management of Health Care Services For Ood Victims: The Case of The Shelter at Nakhon Pathom Rajabhat University Central ThailandДокумент7 страницManagement of Health Care Services For Ood Victims: The Case of The Shelter at Nakhon Pathom Rajabhat University Central ThailandAnonymous C06qenyfkmОценок пока нет
- PDF Applied Failure Analysis 1 NSW - CompressДокумент2 страницыPDF Applied Failure Analysis 1 NSW - CompressAgungОценок пока нет
- Ansi MV Techtopics75 enДокумент2 страницыAnsi MV Techtopics75 enjobpei2Оценок пока нет
- Introduction To Investment AppraisalДокумент43 страницыIntroduction To Investment AppraisalNURAIN HANIS BINTI ARIFFОценок пока нет
- U90 Ladder Tutorial PDFДокумент72 страницыU90 Ladder Tutorial PDFMarlon CalixОценок пока нет
- 6 Elements of A Healthy ChurchДокумент2 страницы6 Elements of A Healthy ChurchJayhia Malaga JarlegaОценок пока нет
- Tapspp0101 PDFДокумент119 страницTapspp0101 PDFAldriel GabayanОценок пока нет
- Claims Reserving With R: Chainladder-0.2.10 Package VignetteДокумент60 страницClaims Reserving With R: Chainladder-0.2.10 Package Vignetteenrique gonzalez duranОценок пока нет
- UN - Towards Sustainable DevelopmentДокумент17 страницUN - Towards Sustainable Developmentviva_33Оценок пока нет