Вам также может понравиться
- Alex Eubank GGIIДокумент40 страницAlex Eubank GGIIOliver Sleiman94% (16)
- D6228 - 10Документ8 страницD6228 - 10POSSDОценок пока нет
- Jeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFДокумент337 страницJeremy A. Greene-Prescribing by Numbers - Drugs and The Definition of Disease-The Johns Hopkins University Press (2006) PDFBruno de CastroОценок пока нет
- Doctors ListДокумент212 страницDoctors ListSaranya Chandrasekar33% (3)
- Reading - On PhonmesДокумент3 страницыReading - On PhonmesNicole CayОценок пока нет
- Linguistics Reading 2Документ11 страницLinguistics Reading 2AlexahaleОценок пока нет
- The StructureДокумент47 страницThe StructureKatrina Sarong AmotoОценок пока нет
- Week 1: Mythology and Folklore English Class Professor: John Michael CulturaДокумент7 страницWeek 1: Mythology and Folklore English Class Professor: John Michael CulturaMichaels CulturaОценок пока нет
- TranscriptionДокумент6 страницTranscriptionDanail MarinovОценок пока нет
- Segmental PhonologyДокумент9 страницSegmental PhonologyJessy AnneОценок пока нет
- Phonology and Phonetics TranscriptionДокумент18 страницPhonology and Phonetics TranscriptionIrving MartínОценок пока нет
- Introduction To LinguisticsДокумент4 страницыIntroduction To LinguisticsRomnick Fernando CoboОценок пока нет
- Intro To Linguistics Soal ZairДокумент2 страницыIntro To Linguistics Soal Zairمحمد نصرؤلОценок пока нет
- The Prosody of Speech: Melody and RhythmДокумент48 страницThe Prosody of Speech: Melody and RhythmRindelene A. CaipangОценок пока нет
- Theoritical of Frameworks The Assimilation Anlysis On Meghan Trainor'S Singing Articulation Through Phonology ApproachДокумент13 страницTheoritical of Frameworks The Assimilation Anlysis On Meghan Trainor'S Singing Articulation Through Phonology ApproachClinton NyaoreОценок пока нет
- Components of LanguageДокумент16 страницComponents of LanguageStânea Irena Diana100% (1)
- Parts of SpeechДокумент11 страницParts of Speechneeraj punjwaniОценок пока нет
- PHNEMEДокумент4 страницыPHNEMEwombadouglasОценок пока нет
- Formal Properties of Language: Form of The MessageДокумент55 страницFormal Properties of Language: Form of The MessagePragyan AgrawalОценок пока нет
- Phonetics and Phonology Are The Two Fields Dedicated To The Study of Human Speech Sounds and Sound StructuresДокумент11 страницPhonetics and Phonology Are The Two Fields Dedicated To The Study of Human Speech Sounds and Sound StructuresKisan SinghОценок пока нет
- Written Versus Spoken EnglishДокумент9 страницWritten Versus Spoken Englishʚϊɞ Sarah Omar ʚϊɞ100% (1)
- 6 ФОНЕТИКАДокумент7 страниц6 ФОНЕТИКАВиктория ДмитренкоОценок пока нет
- In PhoneticsДокумент3 страницыIn Phoneticsbello abubakarОценок пока нет
- Linguistic Literary Terms of AccentologyДокумент1 страницаLinguistic Literary Terms of AccentologyArul DayanandОценок пока нет
- Somatic Idioms RevisitedДокумент5 страницSomatic Idioms RevisitedSohag LTCОценок пока нет
- The Prosody of Speech - Melody and Rhythm - The Handbook of Phonetic Sciences - Blackwell Reference OnlineДокумент22 страницыThe Prosody of Speech - Melody and Rhythm - The Handbook of Phonetic Sciences - Blackwell Reference OnlineHAKAN ÖZTEMÜRОценок пока нет
- Typology: Linguistics Syllables Suprasegmental PhonemicДокумент6 страницTypology: Linguistics Syllables Suprasegmental PhonemicHanie Balmedina-RazoОценок пока нет
- Discourse Analysis and PhonologyДокумент30 страницDiscourse Analysis and Phonologyalfa1411100% (1)
- Challenges To Translate IdiomsДокумент9 страницChallenges To Translate IdiomsOrsi SimonОценок пока нет
- Phonetics Vs Phonemics Written ReportДокумент11 страницPhonetics Vs Phonemics Written ReportDave Dela Cruz AlvarezОценок пока нет
- 7900Документ101 страница7900justlilyОценок пока нет
- Couper Kuhlen 01Документ19 страницCouper Kuhlen 01Kevin JohnsonОценок пока нет
- Question 1Документ15 страницQuestion 1Samson EdunjobiОценок пока нет
- 02chapter 2 SoundДокумент98 страниц02chapter 2 SoundRoger langaОценок пока нет
- How To Create A LanguageДокумент103 страницыHow To Create A Languagesaironwe100% (2)
- CompositionДокумент5 страницCompositionJumberi AmaghlobeliОценок пока нет
- SegmentsДокумент4 страницыSegmentsNikko John de TorresОценок пока нет
- 5 Features of Connected SpeechДокумент7 страниц5 Features of Connected SpeechLovely Deins AguilarОценок пока нет
- Features of Connected SpeechДокумент30 страницFeatures of Connected SpeechJoselyn Wrande Sanhueza100% (2)
- Chapter 2 - Describing Speech SoundsДокумент11 страницChapter 2 - Describing Speech SoundsTearsOfTwoHeartsОценок пока нет
- Lexicology. Lesson 10. STYLISTIC CLASSFICATION OF THE ENGLISH VOCABULARYДокумент35 страницLexicology. Lesson 10. STYLISTIC CLASSFICATION OF THE ENGLISH VOCABULARYIrina CretuОценок пока нет
- Phonetics and PhonologyДокумент29 страницPhonetics and PhonologyVini Dwi PutriОценок пока нет
- How To Create A Language by Pablo David FloresДокумент51 страницаHow To Create A Language by Pablo David Floresaidan wendtОценок пока нет
- Consonant: Consonance and Dissonance Consonant (Band)Документ5 страницConsonant: Consonance and Dissonance Consonant (Band)Gabriel Mariela L.Оценок пока нет
- Phonology PDFДокумент18 страницPhonology PDFSivakumarThangavelОценок пока нет
- Advanced English Grammar with ExercisesОт EverandAdvanced English Grammar with ExercisesРейтинг: 2.5 из 5 звезд2.5/5 (12)
- Лекція 4 Phoneme TheoryДокумент5 страницЛекція 4 Phoneme TheoryОксана ХруникОценок пока нет
- Phonetic TermsДокумент15 страницPhonetic TermsLê Đức ToànОценок пока нет
- Orthographic Words LinguisticДокумент13 страницOrthographic Words LinguisticDaniel WongОценок пока нет
- Seminar 2: Phonetic and Morphological Means of Stylistics 1. Phonetic Means of StylysticsДокумент4 страницыSeminar 2: Phonetic and Morphological Means of Stylistics 1. Phonetic Means of Stylysticsdiiiano4kaОценок пока нет
- Phonology For Listening - Relishing The MessyДокумент15 страницPhonology For Listening - Relishing The MessyNoerdien Ooff De'ring100% (2)
- Phonetics and PhonolgyДокумент14 страницPhonetics and PhonolgyAbdulRehman100% (3)
- English and Arabic Phonology For Transla PDFДокумент17 страницEnglish and Arabic Phonology For Transla PDFAbdel MalekОценок пока нет
- Orthographic Words - LinguisticДокумент13 страницOrthographic Words - LinguisticDavid Vilca0% (1)
- Kortvelyessy Stekauer FINALДокумент28 страницKortvelyessy Stekauer FINALMarcel NowotkoОценок пока нет
- ENG502 Midterm Short NotesДокумент18 страницENG502 Midterm Short NotesRukhshanda NaazОценок пока нет
- Phonetics and Phonology Q&AДокумент7 страницPhonetics and Phonology Q&AsewzeeОценок пока нет
- The Nature of The LanguageДокумент8 страницThe Nature of The LanguageSergio GaticaОценок пока нет
- Phonemes and Allophones - Minimal PairsДокумент5 страницPhonemes and Allophones - Minimal PairsVictor Rafael Mejía Zepeda EDUCОценок пока нет
- Phonetics in Phonology: John J. OhalaДокумент6 страницPhonetics in Phonology: John J. OhalaNoorul JannahОценок пока нет
- Basic Notes Phonetics and PhonologyДокумент26 страницBasic Notes Phonetics and PhonologyAlberto Cravioto100% (5)
- Transcription: IntonationДокумент3 страницыTranscription: IntonationVolkovinszki MihaiОценок пока нет
- Phonology: Handout For Psy 598-02, Summer 2001Документ11 страницPhonology: Handout For Psy 598-02, Summer 2001Ibtessam Hassan KadeebОценок пока нет
- 100 Words Almost Everyone Mixes Up or ManglesОт Everand100 Words Almost Everyone Mixes Up or ManglesРейтинг: 4 из 5 звезд4/5 (3)
- Accoun LeadДокумент2 страницыAccoun LeadJijoОценок пока нет
- (MT Training) Editing Rediscovered PDFДокумент4 страницы(MT Training) Editing Rediscovered PDFJijoОценок пока нет
- Medical Transcription Syllabus Winter 2006Документ15 страницMedical Transcription Syllabus Winter 2006JijoОценок пока нет
- (MT Training) Enhance ProductivityДокумент1 страница(MT Training) Enhance ProductivityJijoОценок пока нет
- (MT Training) Dictation and Transcription PDFДокумент4 страницы(MT Training) Dictation and Transcription PDFJijoОценок пока нет
- (MT Training) Editing Rediscovered PDFДокумент4 страницы(MT Training) Editing Rediscovered PDFJijoОценок пока нет
- Engl SHДокумент4 страницыEngl SHkaluvas44Оценок пока нет
- A Guide To Dealing WithДокумент13 страницA Guide To Dealing WithJijoОценок пока нет
- Professional Levels (MT)Документ3 страницыProfessional Levels (MT)JijoОценок пока нет
- AAMT Registered Medical Transcriptionist (RMT) Exam: Candidate GuideДокумент16 страницAAMT Registered Medical Transcriptionist (RMT) Exam: Candidate GuideJijoОценок пока нет
- Certification Fact SheetДокумент3 страницыCertification Fact SheetJijoОценок пока нет
- American Association For Medical Transcription 100 Sycamore Avenue, Modesto, CA 95354-0550 - 800-982-2182Документ5 страницAmerican Association For Medical Transcription 100 Sycamore Avenue, Modesto, CA 95354-0550 - 800-982-2182JijoОценок пока нет
- Sample CMT CertificateДокумент1 страницаSample CMT CertificateJijoОценок пока нет
- American Association For Medical Transcription 100 Sycamore Avenue, Modesto, CA 95354-0550 - 800-982-2182Документ5 страницAmerican Association For Medical Transcription 100 Sycamore Avenue, Modesto, CA 95354-0550 - 800-982-2182JijoОценок пока нет
- Avoiding CPSEs - Laboratory Medication Vital SignsДокумент30 страницAvoiding CPSEs - Laboratory Medication Vital SignsForОценок пока нет
- Mil STD 792fДокумент13 страницMil STD 792fdoradoanОценок пока нет
- Global Talent MonitorДокумент30 страницGlobal Talent Monitornitinsoni807359Оценок пока нет
- Neurocisticercosis PDFДокумент7 страницNeurocisticercosis PDFFiorella Alexandra HRОценок пока нет
- Ds0h Ufaa68 ProposalДокумент11 страницDs0h Ufaa68 Proposaledward baskaraОценок пока нет
- Basics of Fire SprinklerДокумент21 страницаBasics of Fire SprinklerLeo_1982Оценок пока нет
- PolydactylyДокумент43 страницыPolydactylyWara Samsarga GedeОценок пока нет
- S ELITE Nina Authors Certain Ivey This Reproduce Western Material Management Gupta Names Do OntarioДокумент15 страницS ELITE Nina Authors Certain Ivey This Reproduce Western Material Management Gupta Names Do Ontariocarlos menaОценок пока нет
- ASD Diagnosis Tools - UpToDateДокумент3 страницыASD Diagnosis Tools - UpToDateEvy Alvionita Yurna100% (1)
- Lichens - Naturally Scottish (Gilbert 2004) PDFДокумент46 страницLichens - Naturally Scottish (Gilbert 2004) PDF18Delta100% (1)
- Review - Practical Accounting 1Документ2 страницыReview - Practical Accounting 1Kath LeynesОценок пока нет
- ReliabilityДокумент5 страницReliabilityArmajaya Fajar SuhardimanОценок пока нет
- Big 9 Master SoalДокумент6 страницBig 9 Master Soallilik masrukhahОценок пока нет
- Bio411 C1Документ1 страницаBio411 C1Aqiena BalqisОценок пока нет
- Covid-19 Mitigation PlanДокумент8 страницCovid-19 Mitigation PlanEkum EdunghuОценок пока нет
- ISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixДокумент3 страницыISO 45001:2018 & OHSAS 18001:2007 Clause-Wise Comparison MatrixvenkatesanОценок пока нет
- REV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Документ2 страницыREV Description Appr'D CHK'D Prep'D: Tolerances (Unless Otherwise Stated) - (In)Bacano CapoeiraОценок пока нет
- Gender, Slum Poverty and Climate Change in Flooded River Lines in Metro ManilaДокумент53 страницыGender, Slum Poverty and Climate Change in Flooded River Lines in Metro ManilaADBGADОценок пока нет
- Basic Electrical Engineering NotesДокумент25 страницBasic Electrical Engineering NotesAnas AnsariОценок пока нет
- Turning Risk Into ResultsДокумент14 страницTurning Risk Into Resultsririschristin_171952Оценок пока нет
- Terminologi AnatomiaДокумент49 страницTerminologi AnatomiaLuluk QurrataОценок пока нет
- Care of Clients With Problems in OxygenationДокумент5 страницCare of Clients With Problems in OxygenationSkyla FiestaОценок пока нет
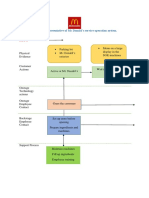
- Blueprint Huynh My Ky Duyen 2022 McDonald'sДокумент2 страницыBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênОценок пока нет
- UK Tax SystemДокумент13 страницUK Tax SystemMuhammad Sajid Saeed100% (1)
- Case Report CMV RetinitisДокумент27 страницCase Report CMV RetinitistaniamaulaniОценок пока нет
- A Comprehensive Review of Cementitious Grouts - Composition, Properties, Requirements and Advanced PerformanceДокумент16 страницA Comprehensive Review of Cementitious Grouts - Composition, Properties, Requirements and Advanced PerformanceiporrasОценок пока нет
- 2022-Brochure Neonatal PiccДокумент4 страницы2022-Brochure Neonatal PiccNAIYA BHAVSARОценок пока нет