Вам также может понравиться
- 2024 Health CalendarДокумент3 страницы2024 Health Calendarlobomho.infoОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- ICD 10 Codes For HIVДокумент2 страницыICD 10 Codes For HIVmahi50Оценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Practice Exam 2 WaterДокумент5 страницPractice Exam 2 WaterSigmund SiyОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
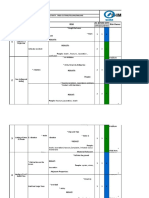
- Hazard Identification and Risk Assessment Control - Tree Cutting & Earth BallingДокумент9 страницHazard Identification and Risk Assessment Control - Tree Cutting & Earth BallingSAMUEL POBREОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Occupational Health in Aviation PDFДокумент235 страницOccupational Health in Aviation PDFabhayОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Pendidikan, Pekerjaan Dan Pendapatan Terhadap Kejadian Lelaki Seks LelakiДокумент7 страницPendidikan, Pekerjaan Dan Pendapatan Terhadap Kejadian Lelaki Seks LelakiFeny WartisaОценок пока нет
- Merged TDL Files 20210111112759Документ2 страницыMerged TDL Files 20210111112759api-545768247Оценок пока нет
- The Bishop ScoreДокумент3 страницыThe Bishop ScoreJheanAlphonsineT.MeansОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- 2.3 Post Marketing Survaillence - Clinical Research - Pharma DostДокумент7 страниц2.3 Post Marketing Survaillence - Clinical Research - Pharma DostjhancyОценок пока нет
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- MDG Progress Towards MDG 4 and 5Документ25 страницMDG Progress Towards MDG 4 and 5John Thiong'oОценок пока нет
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Literature of AsthmaДокумент23 страницыLiterature of AsthmaAbrar Hendri PutraОценок пока нет
- World Breastfeeding Week 2011Документ20 страницWorld Breastfeeding Week 2011Annapurna DangetiОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The History and Scope of EpidemiologyДокумент40 страницThe History and Scope of EpidemiologyMike LorenaОценок пока нет
- Customer Perception of Health Insurance PDFДокумент14 страницCustomer Perception of Health Insurance PDFRajesh Singh KumabamОценок пока нет
- Breast Cancer Screening: Iarc Handbooks of Cancer PreventionДокумент481 страницаBreast Cancer Screening: Iarc Handbooks of Cancer PreventionLary AlexandraОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Upshot 4 13Документ2 страницыUpshot 4 13aslesiccamperОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Data Upload ShopeeДокумент28 страницData Upload Shopeebanyakmauu borОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Monthly Report Form For NDP Edited 2 From PHTДокумент1 страницаMonthly Report Form For NDP Edited 2 From PHTAnthony Zuniega0% (1)
- Block 1 PDFДокумент388 страницBlock 1 PDFShubham ShuklaОценок пока нет
- Quotes On MicrobiologyДокумент39 страницQuotes On MicrobiologyTummalapalli Venkateswara Rao100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Delta Air Lines Internship ProjectДокумент4 страницыDelta Air Lines Internship Projectapi-543821814Оценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- Kathmandu University School of Medical Sciences Dhulikhel, KavreДокумент43 страницыKathmandu University School of Medical Sciences Dhulikhel, Kavrerojina poudelОценок пока нет
- Sv801 Swasthavritta - I 4-0-0-4 Concept of Ahara, Vihara and Rasayanam in HealthДокумент2 страницыSv801 Swasthavritta - I 4-0-0-4 Concept of Ahara, Vihara and Rasayanam in HealthanuОценок пока нет
- Global Health Indicators - An OverviewДокумент2 страницыGlobal Health Indicators - An OverviewAnnisa AlkhairiyahОценок пока нет
- Universal Health Care Implementers Project - GuidelinesДокумент3 страницыUniversal Health Care Implementers Project - GuidelinesErnest Jerome Malamion0% (3)
- Materi P5MДокумент14 страницMateri P5MHariyanto oknesОценок пока нет
- Report On The Global Statistical Data of COVIDДокумент3 страницыReport On The Global Statistical Data of COVIDChristian Angelo G. MontigoОценок пока нет
- COVID-19 mRNA Vaccines: Lessons Learned From The Registrational Trials and Global Vaccination CampaignДокумент38 страницCOVID-19 mRNA Vaccines: Lessons Learned From The Registrational Trials and Global Vaccination CampaignGabriela PachecoОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Proof The Covid-19 Jabs Should Be Stopped NowДокумент2 страницыProof The Covid-19 Jabs Should Be Stopped NowDiogo MiguelОценок пока нет
- Water Reuse in Developing Countries: The Golden Rule of Wastewater ReuseДокумент12 страницWater Reuse in Developing Countries: The Golden Rule of Wastewater ReuseHanna SilverioОценок пока нет