Вам также может понравиться
- Poster Session II: ConclusionДокумент1 страницаPoster Session II: ConclusionjuniorebindaОценок пока нет
- Fluid Management - Presentation PDFДокумент16 страницFluid Management - Presentation PDFjuniorebinda100% (1)
- CD001450Документ98 страницCD001450juniorebindaОценок пока нет
- Bronchiolitis PDFДокумент5 страницBronchiolitis PDFjuniorebindaОценок пока нет
- g4 Paeds 2012 RosterДокумент7 страницg4 Paeds 2012 RosterjuniorebindaОценок пока нет
- Psychological Management of Cystic FibrosisДокумент10 страницPsychological Management of Cystic FibrosisjuniorebindaОценок пока нет
- Paeds Ebm Assignment Gemp4 PDFДокумент7 страницPaeds Ebm Assignment Gemp4 PDFjuniorebindaОценок пока нет
- Immunisation 2013 PDFДокумент1 страницаImmunisation 2013 PDFjuniorebindaОценок пока нет
- Paeds Ebm Assignment Template Gemp4Документ7 страницPaeds Ebm Assignment Template Gemp4juniorebindaОценок пока нет
- Student Guide For Chronic Patient Attachment - 2011Документ6 страницStudent Guide For Chronic Patient Attachment - 2011juniorebindaОценок пока нет
- 21 Obstetric Anaesthesia PDFДокумент0 страниц21 Obstetric Anaesthesia PDFjuniorebindaОценок пока нет
- End of Year Examination 2009 SACS: RD THДокумент21 страницаEnd of Year Examination 2009 SACS: RD THjuniorebindaОценок пока нет
- Chronic Patient Portfolio Marking Rubric PDFДокумент1 страницаChronic Patient Portfolio Marking Rubric PDFjuniorebindaОценок пока нет
- Challenges in Care of Adult CF Patients - The Specialist Cystic Fibrosis TeamДокумент4 страницыChallenges in Care of Adult CF Patients - The Specialist Cystic Fibrosis TeamjuniorebindaОценок пока нет
- CVS MCQ 2010 PDFДокумент23 страницыCVS MCQ 2010 PDFjuniorebinda60% (5)
- Final Forensic Medicine Anaesthesia Emergency Medicine TraumaДокумент7 страницFinal Forensic Medicine Anaesthesia Emergency Medicine TraumajuniorebindaОценок пока нет
- 20 Endocrine Disease and AnaesthesiaДокумент0 страниц20 Endocrine Disease and AnaesthesiajuniorebindaОценок пока нет
- Epidural AnaesthesiaДокумент13 страницEpidural AnaesthesiajuniorebindaОценок пока нет
- 19 Respiratory Renal and Hepatic Disease and AnaesthesiaДокумент0 страниц19 Respiratory Renal and Hepatic Disease and AnaesthesiajuniorebindaОценок пока нет
- 16 Complications in Anaesthesia PDFДокумент0 страниц16 Complications in Anaesthesia PDFjuniorebindaОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Health Assessment in Nursing Weber 5th Edition Test BankДокумент9 страницHealth Assessment in Nursing Weber 5th Edition Test BankSpencerMoorenbds100% (35)
- Diagnostic Tests PDFДокумент2 страницыDiagnostic Tests PDFBenedict AlvarezОценок пока нет
- Putney Rehab Centre TimetableДокумент2 страницыPutney Rehab Centre Timetableapi-280584977Оценок пока нет
- Newly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterДокумент4 страницыNewly Diagnosed HIV Cases in The Philippines: National Epidemiology CenterJonas BagasОценок пока нет
- Dra Juson Labor & DeliveryДокумент153 страницыDra Juson Labor & DeliveryaringkinkingОценок пока нет
- Nurs FPX 4030 Assessment 3 Pico T Questions and An Evidence Based ApproachДокумент5 страницNurs FPX 4030 Assessment 3 Pico T Questions and An Evidence Based ApproachEmma WatsonОценок пока нет
- El Papiro de Edwin Smith y Su TrascendenДокумент6 страницEl Papiro de Edwin Smith y Su TrascendenSebastian PintoОценок пока нет
- Gotthard Bulau Closed Water-Seal Drainage For Empyema,: John A. MeyerДокумент3 страницыGotthard Bulau Closed Water-Seal Drainage For Empyema,: John A. Meyerputri aprilianiОценок пока нет
- Will The Speed of COVID-19-vaccine Development Reset Industry NormsДокумент7 страницWill The Speed of COVID-19-vaccine Development Reset Industry NormsraytjanОценок пока нет
- Annex 1 RSWITCH - Informed Consent - Forms - EnglishДокумент6 страницAnnex 1 RSWITCH - Informed Consent - Forms - Englishmerealemketema1Оценок пока нет
- Introduction To Electronic Medical RecordsДокумент16 страницIntroduction To Electronic Medical RecordsSaniat Obaidullah100% (1)
- Chapter 38 - Management of Patients With Intestinal and Rectal DisordersДокумент7 страницChapter 38 - Management of Patients With Intestinal and Rectal DisordersMichael BoadoОценок пока нет
- Upper Extremity Reconstruction: Surgical SolutionsДокумент16 страницUpper Extremity Reconstruction: Surgical Solutionsapi-488115640Оценок пока нет
- Child Assessment Tool FinalДокумент16 страницChild Assessment Tool FinalmanigottagetthisdoneОценок пока нет
- Case of Grade 4 Bedsore Over Sacral Region With Management A Case ReportДокумент3 страницыCase of Grade 4 Bedsore Over Sacral Region With Management A Case ReportAmna AliОценок пока нет
- Ectopic Pregnancy (m104)Документ13 страницEctopic Pregnancy (m104)Alphine DalgoОценок пока нет
- Lower Extremity AmputationsДокумент42 страницыLower Extremity Amputationsalinutza_childОценок пока нет
- Csi Cardiology Update 2018 Binder 1Документ1 160 страницCsi Cardiology Update 2018 Binder 1nikhil100% (1)
- Hajj Health Requirements English LanguageДокумент8 страницHajj Health Requirements English Languageelis suryaniОценок пока нет
- Our Noble and Beloved Carroll DunhamДокумент2 страницыOur Noble and Beloved Carroll Dunhamkrishna2205Оценок пока нет
- Research Critiques and PICOT QuestionДокумент10 страницResearch Critiques and PICOT QuestionSamwel KangyОценок пока нет
- HemoglobinopathiesДокумент10 страницHemoglobinopathiespriscillaОценок пока нет
- Aiims Part IiiДокумент104 страницыAiims Part IiiMourian AmanОценок пока нет
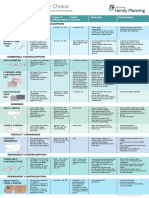
- Contraception Options in New ZealandДокумент2 страницыContraception Options in New ZealandStuff NewsroomОценок пока нет
- Artificial Respiration: ForceДокумент15 страницArtificial Respiration: Forcekushal NeupaneОценок пока нет
- Portion Medical Primary Care Health CentersДокумент21 страницаPortion Medical Primary Care Health CenterssdardaОценок пока нет
- Primay Health CentresДокумент100 страницPrimay Health CentresBirupakshya RoutОценок пока нет
- WHO MHGap Guide English PDFДокумент121 страницаWHO MHGap Guide English PDFYolanda Dwi OktaviyaniОценок пока нет
- MK SurgeryДокумент900 страницMK Surgerybovarep216Оценок пока нет
- RCSI Bahrain ConnectED Newsletter Winter 2022-23Документ32 страницыRCSI Bahrain ConnectED Newsletter Winter 2022-23Yousif YousifОценок пока нет