Вам также может понравиться
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 0 Act Sunum 2020 NewwДокумент58 страниц0 Act Sunum 2020 NewwPınar AdsızОценок пока нет
- Zelio Control Relays - RM22TR33Документ7 страницZelio Control Relays - RM22TR33SIVARAMANJAGANATHANОценок пока нет
- Preventive Pump SetДокумент67 страницPreventive Pump Setwtpstp sardОценок пока нет
- Board of Technical Education Uttar Pradesh Lucknow: CODE 2298Документ2 страницыBoard of Technical Education Uttar Pradesh Lucknow: CODE 2298Md Shaaz100% (1)
- Art 16-18Документ528 страницArt 16-18ErudíhenОценок пока нет
- Grade 7 Information Writing: The Bulldog: A Dog Like No OtherДокумент5 страницGrade 7 Information Writing: The Bulldog: A Dog Like No Otherapi-202727113Оценок пока нет
- SC607 Assignment2Документ2 страницыSC607 Assignment2Tirthankar AdhikariОценок пока нет
- NL0520 NEPAL SagarmathaДокумент12 страницNL0520 NEPAL SagarmathaPrashantpal RaiОценок пока нет
- Pharma Iii To Viii PDFДокумент57 страницPharma Iii To Viii PDFRaja PrabhuОценок пока нет
- S120 Technical Specifications - 23 Dec 21Документ17 страницS120 Technical Specifications - 23 Dec 21jayraj jadejaОценок пока нет
- "Chapter 9 - Influence Lines For Statically Determinate Structures" in "Structural Analysis" On Manifold @tupressДокумент33 страницы"Chapter 9 - Influence Lines For Statically Determinate Structures" in "Structural Analysis" On Manifold @tupressrpsirОценок пока нет
- Comparison of Ozone Vs Uv in WaterДокумент1 страницаComparison of Ozone Vs Uv in WaterRajesh PandeyОценок пока нет
- Unusual and Marvelous MapsДокумент33 страницыUnusual and Marvelous MapsRajarajan100% (1)
- Hipertensiunea Arteriala - Cauze Si TratamenteДокумент25 страницHipertensiunea Arteriala - Cauze Si TratamenteClaudia MurguОценок пока нет
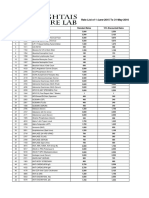
- Rate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesДокумент25 страницRate List of 1-June-2015 To 31-May-2016: S.No Code Test Name Standard Rates 15% Discounted RatesMirza BabarОценок пока нет
- Statistical Mechanics PDFДокумент578 страницStatistical Mechanics PDFraymon6666100% (6)
- Civil 416Документ2 страницыCivil 416tskh11Оценок пока нет
- Elevator ControlДокумент3 страницыElevator ControlNATHANОценок пока нет
- DalmatiaДокумент265 страницDalmatiaomissam2Оценок пока нет
- Essenza Refurbished Siemens MRI MachineДокумент2 страницыEssenza Refurbished Siemens MRI Machinetech.arnicahealthОценок пока нет
- German Din Vde Standards CompressДокумент3 страницыGerman Din Vde Standards CompressYurii SlipchenkoОценок пока нет
- ASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFДокумент5 страницASTM E 1066 - 95 Standard Practice For Ammonia Colorimetric Leak Testing PDFАртем ТитовОценок пока нет
- Telmisartan, ISMNДокумент8 страницTelmisartan, ISMNDenise EspinosaОценок пока нет
- History of Journalism With Whiteboard StyleДокумент56 страницHistory of Journalism With Whiteboard StyleXeon JupiterОценок пока нет
- Alien Magic - William Hamilton IIIДокумент179 страницAlien Magic - William Hamilton IIICarlos Rodriguez100% (7)
- Power System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustДокумент10 страницPower System Analysis and Design EE-461: Tassawar Kazmi Lecturer, EE Department, Seecs, NustShahab SaqibОценок пока нет
- MPDFДокумент5 страницMPDFRoyalAryansОценок пока нет
- Lesson 4Документ10 страницLesson 4Nagiri MuraliОценок пока нет
- Antena Kathrein 742266 PDFДокумент2 страницыAntena Kathrein 742266 PDFcesarbayonaОценок пока нет
- 2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairДокумент6 страниц2017 Hyundai Sonata L4-2.4L Engine Controls (Powertrain Management) - ALLDATA RepairChino PlagaОценок пока нет