Вам также может понравиться
- Enagic KW2 PDFДокумент125 страницEnagic KW2 PDFKS Lee100% (6)
- Cancer Protocol - EnglishДокумент7 страницCancer Protocol - Englishchouette cool100% (1)
- Heidenreich Et Al. - Anatomic Extent of Pelvic Lymphadenectomy in Bladder CancerДокумент5 страницHeidenreich Et Al. - Anatomic Extent of Pelvic Lymphadenectomy in Bladder CanceryuenkeithОценок пока нет
- Current Opinion On Lymphadenectomy in Pancreatic Cancer SurgeryДокумент5 страницCurrent Opinion On Lymphadenectomy in Pancreatic Cancer Surgeryyacine26Оценок пока нет
- Acs 06 02 152Документ7 страницAcs 06 02 152crsscribdОценок пока нет
- Tratamiento Esofago Cervical Mendenhall 1994Документ13 страницTratamiento Esofago Cervical Mendenhall 1994Carlos N. Rojas PuyolОценок пока нет
- Surg Apprach EsophagectomyДокумент3 страницыSurg Apprach EsophagectomyDumitru RadulescuОценок пока нет
- Laparoscopic Surgery in Gynaecologic OncologyДокумент7 страницLaparoscopic Surgery in Gynaecologic OncologyManan BoobОценок пока нет
- Periampullary CarcinomaДокумент35 страницPeriampullary Carcinomaminnalesri100% (2)
- Surgical Approaches To Esophageal CancerДокумент6 страницSurgical Approaches To Esophageal CancerYacine Tarik AizelОценок пока нет
- General Consideration in EsophagectomyДокумент4 страницыGeneral Consideration in EsophagectomyDabessa MosissaОценок пока нет
- Artigo 4Документ6 страницArtigo 4gdaraujoОценок пока нет
- 1 s2.0 S0065341116000038 MainДокумент12 страниц1 s2.0 S0065341116000038 MainFlorin AchimОценок пока нет
- Radical Surgery For Cancer of The Pancreas: Kothaj PДокумент3 страницыRadical Surgery For Cancer of The Pancreas: Kothaj Pyacine26Оценок пока нет
- Laparoscopic Resection of Rectal CancerДокумент4 страницыLaparoscopic Resection of Rectal CancerhoangducnamОценок пока нет
- Modified Technique of Radical Inguinal Lymphadenectomy For Penile Carcinoma: Morbidity and OutcomeДокумент7 страницModified Technique of Radical Inguinal Lymphadenectomy For Penile Carcinoma: Morbidity and OutcomeAlwin PrasetyaОценок пока нет
- Oesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHДокумент50 страницOesophageal Carcinoma: Dr. Malghalara Khan PGR, Surgical D Unit, KTHMalgh Kh100% (2)
- Adjuvant Therapy. Most Studies HaveДокумент9 страницAdjuvant Therapy. Most Studies HaveAnonymous UTUWFODCEYОценок пока нет
- 6 Neck DissectionДокумент9 страниц6 Neck DissectionAnne MarieОценок пока нет
- 7897-Article Text-31281-3-10-20181219 PDFДокумент7 страниц7897-Article Text-31281-3-10-20181219 PDFChater WafaОценок пока нет
- Optimal Bowel Resection Margin in Colon Cancer Surgery 2023Документ13 страницOptimal Bowel Resection Margin in Colon Cancer Surgery 2023CIRUGÍA ONCOLÓGICA ABDOMENОценок пока нет
- ABC - Oral CancerДокумент4 страницыABC - Oral Cancerdewishinta12Оценок пока нет
- Controversies in Abdominoperineal Excision: Torbjörn HolmДокумент19 страницControversies in Abdominoperineal Excision: Torbjörn HolmPriscilla Rockbrand CamposОценок пока нет
- Samphire2003 PDFДокумент9 страницSamphire2003 PDFYacine Tarik AizelОценок пока нет
- Esophageal Tumors: Dr. Yusmaidi, SPB - KBDДокумент36 страницEsophageal Tumors: Dr. Yusmaidi, SPB - KBDbahtiarhabibiОценок пока нет
- Squamous Cell Tumors Bile Duct Cancers: PathophysiologyДокумент6 страницSquamous Cell Tumors Bile Duct Cancers: PathophysiologySiti RahmahОценок пока нет
- Surgical Management of Rectal Carcinoma - MILES PROCДокумент5 страницSurgical Management of Rectal Carcinoma - MILES PROCdptkomangОценок пока нет
- Review Article: Intersphincteric Resection and Coloanal Anastomosis in Treatment of Distal Rectal CancerДокумент10 страницReview Article: Intersphincteric Resection and Coloanal Anastomosis in Treatment of Distal Rectal CancerJaysonGarabilesEspejoОценок пока нет
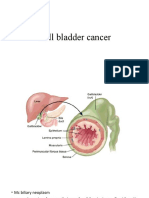
- Gall Bladder CancerДокумент29 страницGall Bladder CancerJoju SebastianОценок пока нет
- Radical Cystectomy: History of The ProcedureДокумент6 страницRadical Cystectomy: History of The ProcedureIvy MinaОценок пока нет
- Ampullary Carcinoma: Treatment and PrognosisДокумент24 страницыAmpullary Carcinoma: Treatment and PrognosisHugo Alves100% (1)
- 46-Endoscopic Laser Excision of Laryngeal CarcinomaДокумент7 страниц46-Endoscopic Laser Excision of Laryngeal Carcinomaedohermendy_32666011Оценок пока нет
- Anterior Resection With Low AnastomosisДокумент10 страницAnterior Resection With Low AnastomosisOhana S.Оценок пока нет
- Tratamentul Cancerului RectalДокумент5 страницTratamentul Cancerului RectalLarisa StanОценок пока нет
- Adenocarcinoma of The Gastroesophageal JunctionДокумент8 страницAdenocarcinoma of The Gastroesophageal JunctionKiara GovenderОценок пока нет
- Carcinoma Maxillary Sinus : of TheДокумент6 страницCarcinoma Maxillary Sinus : of TheInesОценок пока нет
- Role of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomaДокумент8 страницRole of Percutaneous Ultrasonographic Guided Radiofrequency Ablation in The Management of Hepatocellular CarcinomadickyaririsandyОценок пока нет
- 2021 Recomendations For Srveillance and Manangemnt of Recurrent Esophageal Cancer Following Endoscopic TherapiesДокумент12 страниц2021 Recomendations For Srveillance and Manangemnt of Recurrent Esophageal Cancer Following Endoscopic TherapiesykommОценок пока нет
- Splenic Hilar DissectionДокумент12 страницSplenic Hilar Dissectionnsv.epicОценок пока нет
- Figure 1A: Dr. William BruggeДокумент5 страницFigure 1A: Dr. William BruggeAbrar SabawiОценок пока нет
- Gine 2Документ9 страницGine 2Cimpean SorinОценок пока нет
- Celiac Lymph Node Resection and Porta Hepatis DiseaseДокумент6 страницCeliac Lymph Node Resection and Porta Hepatis DiseaseAndreeaPopescuОценок пока нет
- Retroperitoneal Nodal Metastases From Colorectal Cancer: Curable Metastases With Radical Retroperitoneal Lymphadenectomy in Selected PatientsДокумент8 страницRetroperitoneal Nodal Metastases From Colorectal Cancer: Curable Metastases With Radical Retroperitoneal Lymphadenectomy in Selected PatientsSchiopu VictorОценок пока нет
- World's Largest Science, Technology & Medicine Open Access Book PublisherДокумент24 страницыWorld's Largest Science, Technology & Medicine Open Access Book PublisherIon MoisescuОценок пока нет
- Management of Primary Testicular Tumor: Alireza Ghoreifi,, Hooman DjaladatДокумент7 страницManagement of Primary Testicular Tumor: Alireza Ghoreifi,, Hooman DjaladatfelipeОценок пока нет
- Acalasia - TratamientoДокумент6 страницAcalasia - TratamientoManuel MontellanosОценок пока нет
- Radioguided Sentinel Lymph Node Biopsy in Breast Cancer SurgeryДокумент18 страницRadioguided Sentinel Lymph Node Biopsy in Breast Cancer Surgerybickxy_katiОценок пока нет
- 2017 Surgical Evolution of Rectal CancerДокумент8 страниц2017 Surgical Evolution of Rectal CancerDr Juan Antonio Villanueva (Coloproctologia)Оценок пока нет
- 04 Esophageal TumorsДокумент36 страниц04 Esophageal TumorsDetty NoviantyОценок пока нет
- ATAR O Ocampo 2014 PJSSДокумент11 страницATAR O Ocampo 2014 PJSSPrince VallejosОценок пока нет
- Perkutana AblacijaДокумент7 страницPerkutana AblacijaNenad DjokicОценок пока нет
- Sub-Adventitial Divestment Technique For Resecting Artery-Involved Pancreatic Cancer: A Retrospective Cohort StudyДокумент11 страницSub-Adventitial Divestment Technique For Resecting Artery-Involved Pancreatic Cancer: A Retrospective Cohort StudyMatias Jurado ChaconОценок пока нет
- Minimally Invasive Surgery For Esophageal Cancer: Review of The Literature and Institutional ExperienceДокумент8 страницMinimally Invasive Surgery For Esophageal Cancer: Review of The Literature and Institutional ExperienceNurulArifahAmirОценок пока нет
- Pelvic and Paraaortic Lymphadenectomy in Gynecologic Cancers - UpToDateДокумент31 страницаPelvic and Paraaortic Lymphadenectomy in Gynecologic Cancers - UpToDateAMGY82100% (1)
- Laparoscopic Versus Open Transhiatal Esophagectomy For Distal and Junction CancerДокумент6 страницLaparoscopic Versus Open Transhiatal Esophagectomy For Distal and Junction CancerDea Melinda SabilaОценок пока нет
- Breast Cancer Study Case PDFДокумент8 страницBreast Cancer Study Case PDFLuna LinОценок пока нет
- RJX 102Документ3 страницыRJX 102FachryОценок пока нет
- 2021 Techniques of Esophageal Anastomosis For EsophagectomyДокумент14 страниц2021 Techniques of Esophageal Anastomosis For EsophagectomyykommОценок пока нет
- Clinicopathological Features and Treatment OutcomeДокумент9 страницClinicopathological Features and Treatment Outcomesyfs92ctpvОценок пока нет
- BladderДокумент36 страницBladderdrsumitavaОценок пока нет
- Case Studies in Advanced Skin Cancer Management: An Osce Viva ResourceОт EverandCase Studies in Advanced Skin Cancer Management: An Osce Viva ResourceОценок пока нет
- Intestinal Adaptation After Massive Intestinal Resection: ReviewДокумент8 страницIntestinal Adaptation After Massive Intestinal Resection: ReviewYacine Tarik AizelОценок пока нет
- Enterocutaneous Fistula: Jennifer D. Stanger and Andreas H. MeierДокумент5 страницEnterocutaneous Fistula: Jennifer D. Stanger and Andreas H. MeierYacine Tarik AizelОценок пока нет
- Matarese2012 PDFДокумент11 страницMatarese2012 PDFYacine Tarik AizelОценок пока нет
- The Etiology of Enterocutaneous Fistula Predicts OutcomeДокумент5 страницThe Etiology of Enterocutaneous Fistula Predicts OutcomeYacine Tarik AizelОценок пока нет
- Owen 2013Документ9 страницOwen 2013Yacine Tarik AizelОценок пока нет
- Optimising The Treatment of Upper Gastrointestinal FistulaeДокумент9 страницOptimising The Treatment of Upper Gastrointestinal FistulaeYacine Tarik AizelОценок пока нет
- Negative Pressure Wound Treatment in The Outpatient Setting: Name of PolicyДокумент26 страницNegative Pressure Wound Treatment in The Outpatient Setting: Name of PolicyYacine Tarik AizelОценок пока нет
- Guideline For The Management of Adult Patients With A High Output StomaДокумент12 страницGuideline For The Management of Adult Patients With A High Output StomaYacine Tarik AizelОценок пока нет
- Piron I 2016Документ13 страницPiron I 2016Yacine Tarik AizelОценок пока нет
- Rnbe-16-0312-Nae High Output Sell SheetДокумент2 страницыRnbe-16-0312-Nae High Output Sell SheetYacine Tarik AizelОценок пока нет
- AIF Questionnaire: Acute Intestinal Failure Special Interest GroupДокумент5 страницAIF Questionnaire: Acute Intestinal Failure Special Interest GroupYacine Tarik AizelОценок пока нет
- 64 1327792215 PDFДокумент4 страницы64 1327792215 PDFYacine Tarik AizelОценок пока нет
- Pi Is 1743919113001738Документ5 страницPi Is 1743919113001738Yacine Tarik AizelОценок пока нет
- Martinez 2007Документ8 страницMartinez 2007Yacine Tarik AizelОценок пока нет
- The Surgical Anatomy and Etiology of Gastrointestinal FistulasДокумент5 страницThe Surgical Anatomy and Etiology of Gastrointestinal FistulasYacine Tarik AizelОценок пока нет
- Vacuum Assisted Closure System in The Management of Enterocutaneous FistulaeДокумент3 страницыVacuum Assisted Closure System in The Management of Enterocutaneous FistulaeYacine Tarik AizelОценок пока нет
- Short Bowel Syndrome AdviceДокумент4 страницыShort Bowel Syndrome AdviceYacine Tarik AizelОценок пока нет
- GCSMC jms2014v3n1p18Документ4 страницыGCSMC jms2014v3n1p18Yacine Tarik AizelОценок пока нет
- WJMH 32 110Документ6 страницWJMH 32 110Yacine Tarik AizelОценок пока нет
- JHBP 24 17Документ7 страницJHBP 24 17Yacine Tarik AizelОценок пока нет
- JTD 08 10 E1136Документ14 страницJTD 08 10 E1136Yacine Tarik AizelОценок пока нет
- Curative Resection For Esophageal Adenocarcinoma: Analysis of 100 en Bloc EsophagectomiesДокумент12 страницCurative Resection For Esophageal Adenocarcinoma: Analysis of 100 en Bloc EsophagectomiesYacine Tarik AizelОценок пока нет
- Cryptorchidism AppendicesДокумент9 страницCryptorchidism AppendicesYacine Tarik AizelОценок пока нет
- Systematized Management of Postoperative Enterocutaneous Fistulas. A 14 Years ExperienceДокумент5 страницSystematized Management of Postoperative Enterocutaneous Fistulas. A 14 Years ExperienceYacine Tarik AizelОценок пока нет
- Cryptorchidism and Its Long-Term ComplicationsДокумент6 страницCryptorchidism and Its Long-Term ComplicationsYacine Tarik AizelОценок пока нет
- Surgical Approaches To Esophageal CancerДокумент6 страницSurgical Approaches To Esophageal CancerYacine Tarik AizelОценок пока нет
- Properties and Therapeutic Application of Bromelain A ReviewДокумент7 страницProperties and Therapeutic Application of Bromelain A ReviewEllisaTanОценок пока нет
- Care of Clients With Problems of The Male Reproductive SystemДокумент18 страницCare of Clients With Problems of The Male Reproductive SystemwakswafuОценок пока нет
- Thyroid Malignancy With MRNDДокумент25 страницThyroid Malignancy With MRNDRashma JosephОценок пока нет
- 1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementДокумент10 страниц1.40 (Surgery) GIT Surgical Diseases - Diagnostics - Obesity ManagementLeo Mari Go LimОценок пока нет
- Cancer Physics Diagnostics Based On Damped Cellular Elastoelectrical Vibrations in Micro Tubules Pokorny 2011Документ13 страницCancer Physics Diagnostics Based On Damped Cellular Elastoelectrical Vibrations in Micro Tubules Pokorny 2011Gabriel KrauskoОценок пока нет
- Down SyndromeДокумент28 страницDown SyndromeChristine LohОценок пока нет
- Immuno Log IДокумент20 страницImmuno Log Idini rustiawatiОценок пока нет
- Recommendations For Cross-Sectional Imaging in Cancer Management, Second EditionДокумент7 страницRecommendations For Cross-Sectional Imaging in Cancer Management, Second EditionNedeljko TrkuljaОценок пока нет
- Neoplasia Outline Notes - PathologyДокумент4 страницыNeoplasia Outline Notes - Pathologykep1313Оценок пока нет
- Persistence Market ResearchДокумент8 страницPersistence Market Researchapi-302003482Оценок пока нет
- Willms TumorДокумент41 страницаWillms TumorBhardwaj Lokesh100% (2)
- Pathology Course Audit-3Документ26 страницPathology Course Audit-3Joana Marie PalatanОценок пока нет
- Solid TumoursДокумент48 страницSolid TumoursViswanadh BОценок пока нет
- Colorectal Cancer Screening: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Документ49 страницColorectal Cancer Screening: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)StangPongritОценок пока нет
- NCMB 312 Finals!Документ25 страницNCMB 312 Finals!Justine Dinice MunozОценок пока нет
- Biostat I Putu Oktayana 18700010Документ61 страницаBiostat I Putu Oktayana 18700010OktaОценок пока нет
- The Pathology of Gastric and Duodenal Polyps: Current ConceptsДокумент19 страницThe Pathology of Gastric and Duodenal Polyps: Current Conceptsaccess pathologicОценок пока нет
- Catat Dan Lat Explanation Text - AbcДокумент3 страницыCatat Dan Lat Explanation Text - AbcDennis StwnОценок пока нет
- HeLa StudyGuide SDSUДокумент29 страницHeLa StudyGuide SDSUFei HuangОценок пока нет
- Approach To The Immunocompromised Patient With Fever and Pulmonary Infiltrates - UpToDateДокумент40 страницApproach To The Immunocompromised Patient With Fever and Pulmonary Infiltrates - UpToDateJúlio ZoéОценок пока нет
- Chapter 2 - VaginaДокумент1 страницаChapter 2 - VaginaalexandrumascanОценок пока нет
- KDIGO Onconeph PT 1 Kidney Impairment and Solid Organ CancerДокумент12 страницKDIGO Onconeph PT 1 Kidney Impairment and Solid Organ CancerMaría MartínezОценок пока нет
- Bioinformatics ManualДокумент117 страницBioinformatics ManualHazo FemberaiОценок пока нет
- Cell Division FORM 4Документ83 страницыCell Division FORM 4sitimarziahОценок пока нет
- Prostate CA Poster SLUДокумент2 страницыProstate CA Poster SLUkar27Оценок пока нет
- Immune Responses, and TransplantationДокумент7 страницImmune Responses, and TransplantationJoyzoeyОценок пока нет
- Ca of The Respiratory System NCM 112 Cell Ab Final TopicsДокумент95 страницCa of The Respiratory System NCM 112 Cell Ab Final TopicsA. Lizette PabloОценок пока нет
- An Introduction To Cancer Biology: When Good Cells Go BadДокумент68 страницAn Introduction To Cancer Biology: When Good Cells Go BadSavitaОценок пока нет