Вам также может понравиться
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansОт EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpОценок пока нет
- Acidosis: Clinical Aspects and Treatment with Isotonic Sodium Bicarbonate SolutionОт EverandAcidosis: Clinical Aspects and Treatment with Isotonic Sodium Bicarbonate SolutionРейтинг: 5 из 5 звезд5/5 (1)
- cASE STUDIES ANSWERДокумент7 страницcASE STUDIES ANSWERNur Liyana0% (1)
- NCA Clinical Laboratory Sciences PDFДокумент40 страницNCA Clinical Laboratory Sciences PDFCoelho Franco100% (1)
- EnzymesДокумент9 страницEnzymesThom TimkangОценок пока нет
- Hemolytic Anemia, SuicideДокумент5 страницHemolytic Anemia, SuicideturkiОценок пока нет
- Test 1 - PSE Model Answers-1Документ3 страницыTest 1 - PSE Model Answers-1Matsiri ImmanuelОценок пока нет
- Module 5Документ31 страницаModule 5xtnreyesОценок пока нет
- 35 Items Saunders Fluids and ElectrolytesДокумент4 страницы35 Items Saunders Fluids and ElectrolytesKrystelle Jade LabineОценок пока нет
- 2 The Use of The Laboratory: 1 Introducing Clinical BiochemistryДокумент2 страницы2 The Use of The Laboratory: 1 Introducing Clinical BiochemistryAmelia PebriantiОценок пока нет
- Standards For Analysis of Cerebrospinal Fluid CSF For XanthochromiaДокумент2 страницыStandards For Analysis of Cerebrospinal Fluid CSF For XanthochromiaanggaririnОценок пока нет
- Aubf Quiz 2Документ8 страницAubf Quiz 2Gene Narune GaronitaОценок пока нет
- 14th BДокумент84 страницы14th BJoy KimОценок пока нет
- Test 1 - APQ Model Answers-1Документ14 страницTest 1 - APQ Model Answers-1Matsiri ImmanuelОценок пока нет
- Theophilus MicrobДокумент4 страницыTheophilus MicrobRaymond NyarkoОценок пока нет
- Dialysis: Cresencio C. Cajigal, Jr. RN, ManДокумент32 страницыDialysis: Cresencio C. Cajigal, Jr. RN, ManMary Jane Avila Bacquial100% (7)
- Worksheet On Nursing Management of Fluid Electrolyte and Acid Base ImbalancesДокумент3 страницыWorksheet On Nursing Management of Fluid Electrolyte and Acid Base ImbalancesMa. Ferimi Gleam BajadoОценок пока нет
- Acute GlomerulonephritisДокумент1 страницаAcute GlomerulonephritisAyrheen FornolesОценок пока нет
- Low Serum Bicarbonate in A Patient With Diabetes&#Документ3 страницыLow Serum Bicarbonate in A Patient With Diabetes&#ayaz ahmadОценок пока нет
- Useful TestsДокумент3 страницыUseful TestsLiamОценок пока нет
- ASCPi Recalls Sep 23 2017Документ3 страницыASCPi Recalls Sep 23 2017Jaine SalongaОценок пока нет
- Case Report: Rapport de CasДокумент3 страницыCase Report: Rapport de CasfadillahidsyamОценок пока нет
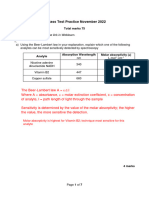
- BM7042 Test Practice Nov 2022 - AnsДокумент7 страницBM7042 Test Practice Nov 2022 - AnsNusra FaizОценок пока нет
- Compre F&EДокумент6 страницCompre F&EArcon AlvarОценок пока нет
- PDF DocumentДокумент4 страницыPDF DocumentAnmol SinghОценок пока нет
- St. Paul University Philippines: School of Health SciencesДокумент8 страницSt. Paul University Philippines: School of Health SciencesJay Andrea Vea IsraelОценок пока нет
- The Serological Investigation of Red Cell Incompatible Transfusion ReactionsДокумент5 страницThe Serological Investigation of Red Cell Incompatible Transfusion ReactionsKAILA SOPHIA CRUZОценок пока нет
- GALAinpregnancyДокумент6 страницGALAinpregnancyumar faruqiОценок пока нет
- Physiology - BSДокумент14 страницPhysiology - BSkep1313Оценок пока нет
- PDF DocumentДокумент4 страницыPDF DocumentAnmol SinghОценок пока нет
- HaematologyДокумент11 страницHaematologyIkram AzmanОценок пока нет
- Case Report of Aspirin Overdose Bezoar Formation and Controversies of Multiple Dose CAДокумент5 страницCase Report of Aspirin Overdose Bezoar Formation and Controversies of Multiple Dose CAAna CortezОценок пока нет
- Urinalysis and Body Fluids - BOC Flashcards - QuizletДокумент37 страницUrinalysis and Body Fluids - BOC Flashcards - QuizlethamoodОценок пока нет
- Physio Multiple Choice Body Fluids and Renal and RespДокумент15 страницPhysio Multiple Choice Body Fluids and Renal and Respsac50900Оценок пока нет
- GROUP 1 - Sweat and UrineДокумент9 страницGROUP 1 - Sweat and Urinechocoholic potchiОценок пока нет
- Clinical MicrosДокумент10 страницClinical Microskthmnts100% (1)
- 2016test 1 - MCQ Model Answers - PharmДокумент14 страниц2016test 1 - MCQ Model Answers - PharmMatsiri ImmanuelОценок пока нет
- Nephrology: I. ProteinuriaДокумент7 страницNephrology: I. ProteinuriaBenjamin NgОценок пока нет
- Case StudyДокумент7 страницCase StudyBilly Belando50% (2)
- Ef 15750Документ144 страницыEf 15750dorjeesengeОценок пока нет
- 14Документ4 страницы14Lyudmyla Gillego0% (1)
- CC Completion Exam Cycle 21Документ6 страницCC Completion Exam Cycle 21Marie LlanesОценок пока нет
- AUBFДокумент32 страницыAUBFAndrei Tumarong AngoluanОценок пока нет
- Offline Grand Test - 1 ExplanationДокумент22 страницыOffline Grand Test - 1 Explanationarun.nayan2013Оценок пока нет
- Fluids PDFДокумент50 страницFluids PDFhuong LОценок пока нет
- Tendency: A To atДокумент5 страницTendency: A To atAdria Putra FarhandikaОценок пока нет
- Specimen Considerations in HematologyДокумент4 страницыSpecimen Considerations in HematologydmclmllОценок пока нет
- GU Blackboard OutlineДокумент15 страницGU Blackboard Outlinedlneisha61Оценок пока нет
- The Role of Organic Acid Analysis in The Diagnosis of Peroxisomal Biogenesis DisordersДокумент4 страницыThe Role of Organic Acid Analysis in The Diagnosis of Peroxisomal Biogenesis DisorderssaranyaОценок пока нет
- AIIMS May 2003 Questions and AnswersДокумент32 страницыAIIMS May 2003 Questions and AnswersSayeed KhanОценок пока нет
- Buchta 2003Документ7 страницBuchta 2003lbОценок пока нет
- Urinalysis Case StudiesДокумент11 страницUrinalysis Case Studiesdandooshe38% (13)
- Practical Use of Urinary Fractional Excretion (In Horses)Документ5 страницPractical Use of Urinary Fractional Excretion (In Horses)July Paulin BarraganОценок пока нет
- CM Recallsss PDFДокумент8 страницCM Recallsss PDFAnne MorenoОценок пока нет
- Fluids, Electrolytes, Acid-Base Disorders, and Nutrition SupportДокумент56 страницFluids, Electrolytes, Acid-Base Disorders, and Nutrition SupportFarryrazaОценок пока нет
- Hypokalemic NephropathyДокумент7 страницHypokalemic NephropathyGoris HariyadiОценок пока нет
- Na Hypo PHA Type IДокумент5 страницNa Hypo PHA Type Ianderson roberto oliveira de sousaОценок пока нет
- Macroscopic Urinalysis, Performed Manually Using Bayer MultistixДокумент12 страницMacroscopic Urinalysis, Performed Manually Using Bayer MultistixKevin TranОценок пока нет
- CC Compre Exam (Pre Internship)Документ7 страницCC Compre Exam (Pre Internship)Marry Grace CiaОценок пока нет
- SUMMATIVEs X POST-RATIOs (Taylor's Version)Документ35 страницSUMMATIVEs X POST-RATIOs (Taylor's Version)JUNAH BIGORNIAОценок пока нет
- BTBC405IU - Lecture Note 3 - Student PDFДокумент25 страницBTBC405IU - Lecture Note 3 - Student PDFPhú NguyễnОценок пока нет
- Preview PDFДокумент103 страницыPreview PDFPhú NguyễnОценок пока нет
- 03-Tools For Healthy Diet-Nutritional Biochemistry 20201008 PDFДокумент19 страниц03-Tools For Healthy Diet-Nutritional Biochemistry 20201008 PDFPhú NguyễnОценок пока нет
- Organic Chemistry Laboratory: Report 5: Simple DistillationДокумент8 страницOrganic Chemistry Laboratory: Report 5: Simple DistillationPhú NguyễnОценок пока нет
- Organic Chemistry Laboratory: Report 7: Liquid-Liquid ExtractionДокумент7 страницOrganic Chemistry Laboratory: Report 7: Liquid-Liquid ExtractionPhú NguyễnОценок пока нет
- Lab 2 CosДокумент4 страницыLab 2 CosPhú NguyễnОценок пока нет
- Organic Chemistry Laboratory: Report 4: Column ChromatographyДокумент5 страницOrganic Chemistry Laboratory: Report 4: Column ChromatographyPhú NguyễnОценок пока нет
- Melting Point: Point at Which Solid and Liquid Phases Are in EquilibriumДокумент6 страницMelting Point: Point at Which Solid and Liquid Phases Are in EquilibriumPhú NguyễnОценок пока нет
- Organic Chemistry Laboratory: Report 8: Fischer Ester SynthesisДокумент7 страницOrganic Chemistry Laboratory: Report 8: Fischer Ester SynthesisPhú NguyễnОценок пока нет
- Subject: Organic chemistry laboratory. Lab partner: Lê Hồ Thi Đỗ Trương Anh Thư Bùi Hữu Đức Trần Hoàng Thanh Tuyền Instructor's name: Dr. Hoang Le SonДокумент46 страницSubject: Organic chemistry laboratory. Lab partner: Lê Hồ Thi Đỗ Trương Anh Thư Bùi Hữu Đức Trần Hoàng Thanh Tuyền Instructor's name: Dr. Hoang Le SonPhú NguyễnОценок пока нет
- ORGANIC CHEMISTRY LABORATORY - Lab 2Документ10 страницORGANIC CHEMISTRY LABORATORY - Lab 2Phú NguyễnОценок пока нет
- Assignment 1 - NguyenTanPhuBTBCIU16057Документ4 страницыAssignment 1 - NguyenTanPhuBTBCIU16057Phú NguyễnОценок пока нет
- Pharmaceutics 12 00264 v2 PDFДокумент30 страницPharmaceutics 12 00264 v2 PDFPhú NguyễnОценок пока нет
- Organic Chemistry Laboratory: Report 6: Reflux ReactionДокумент7 страницOrganic Chemistry Laboratory: Report 6: Reflux ReactionPhú NguyễnОценок пока нет
- ActivitiesДокумент1 страницаActivitiesPhú NguyễnОценок пока нет
- Organic Chemistry Laboratory: Report 3: Thin Layer ChromatographyДокумент7 страницOrganic Chemistry Laboratory: Report 3: Thin Layer ChromatographyPhú NguyễnОценок пока нет
- NUTRACEUTICALS LABORATORY Lab 2Документ10 страницNUTRACEUTICALS LABORATORY Lab 2Phú NguyễnОценок пока нет
- Quiz 1Документ4 страницыQuiz 1Hằng Thanh0% (1)
- Silvestre Dissertation 2019 PDFДокумент353 страницыSilvestre Dissertation 2019 PDFPhú NguyễnОценок пока нет
- Assignment 2 Fermentation PDFДокумент2 страницыAssignment 2 Fermentation PDFPhú NguyễnОценок пока нет
- Nutraceuticals Laboratory Report 3: Determination of Total Flavonoid ContentДокумент7 страницNutraceuticals Laboratory Report 3: Determination of Total Flavonoid ContentPhú NguyễnОценок пока нет
- Citation 221912898Документ1 страницаCitation 221912898Phú NguyễnОценок пока нет
- Mibi FinalДокумент3 страницыMibi FinalPhú NguyễnОценок пока нет
- Nutralab Ex4 Report 1 PDFДокумент10 страницNutralab Ex4 Report 1 PDFPhú NguyễnОценок пока нет
- Ethics of Research Using Hybrids, Chimeras and Cytoplasmic Hybrids?Документ7 страницEthics of Research Using Hybrids, Chimeras and Cytoplasmic Hybrids?Phú NguyễnОценок пока нет
- Solution HW1Документ4 страницыSolution HW1Phú NguyễnОценок пока нет
- Solution Quiz 1Документ2 страницыSolution Quiz 1Phú NguyễnОценок пока нет
- READINGДокумент5 страницREADINGPhú NguyễnОценок пока нет
- Solution HW2Документ4 страницыSolution HW2Phú NguyễnОценок пока нет
- Quiz 2Документ1 страницаQuiz 2Phú NguyễnОценок пока нет
- Answers To Case StudiesДокумент7 страницAnswers To Case StudiesPhú NguyễnОценок пока нет
- Self-Assessment Colour Review of Small Animal Soft Tissue SurgeryДокумент194 страницыSelf-Assessment Colour Review of Small Animal Soft Tissue Surgerymiliindianu100% (3)
- 5 - Endocrinology Passmedicine Q. Bank PART I 2017Документ366 страниц5 - Endocrinology Passmedicine Q. Bank PART I 2017'محمد علي' محمد لافي100% (1)
- Metabolic Complications of Endocrine Surgery in Companion AnimalsДокумент22 страницыMetabolic Complications of Endocrine Surgery in Companion AnimalsEduardo PalaciosОценок пока нет
- Chemical Pathology 5 - HypoglycaemiaДокумент10 страницChemical Pathology 5 - HypoglycaemiaaОценок пока нет
- Hypoglycemia in Adults Without Diabetes Mellitus - Diagnostic Approach - UpToDateДокумент19 страницHypoglycemia in Adults Without Diabetes Mellitus - Diagnostic Approach - UpToDateRaiya MallickОценок пока нет
- Diabetes Mellitus ComplicationДокумент40 страницDiabetes Mellitus ComplicationHathorОценок пока нет
- Https Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId HK9UQ4C5ZEZ7ICEuNXmyPwДокумент8 страницHttps Tdiagnostics - Telangana.gov - in ViewFiles - Aspx ReportId HK9UQ4C5ZEZ7ICEuNXmyPwKuncham LakshmiОценок пока нет
- Pancreatic Solid LeasionsДокумент24 страницыPancreatic Solid LeasionsEliza CrăciunОценок пока нет
- Cystic LesionsДокумент101 страницаCystic LesionsKartik GuptaОценок пока нет
- 7325-300 C-Peptide & Insulin AccuBind VAST ELISA Rev 6Документ2 страницы7325-300 C-Peptide & Insulin AccuBind VAST ELISA Rev 6Luisa MaríaОценок пока нет
- HBP MCQsДокумент67 страницHBP MCQsNessreen JamalОценок пока нет
- Case Studies in CC1Документ12 страницCase Studies in CC1Kayne Viernes67% (18)
- DIABETES MCQsДокумент82 страницыDIABETES MCQsFatima Zuhra100% (2)
- InsulinomaДокумент18 страницInsulinomaBetta BeTta0% (1)
- Endocrinology - Review NotesДокумент9 страницEndocrinology - Review NotesRoa Al-SajjanОценок пока нет
- Diabetes Mellitus: DefinitionДокумент54 страницыDiabetes Mellitus: DefinitionislamnourОценок пока нет
- Althea NCM 116aДокумент192 страницыAlthea NCM 116aspain michaelisОценок пока нет
- PosterДокумент32 страницыPosterBeny RiliantoОценок пока нет
- Jcem 0709Документ20 страницJcem 0709Rao Rizwan ShakoorОценок пока нет
- Generic Name:: Is Used To Dissolve (Cholesterol) Gallstones and PДокумент9 страницGeneric Name:: Is Used To Dissolve (Cholesterol) Gallstones and PZAY EMОценок пока нет
- Antidiabetic Drugs: Raymund N. Tapaoan, RPHДокумент23 страницыAntidiabetic Drugs: Raymund N. Tapaoan, RPHNicole EncinaresОценок пока нет
- Gastrinomas Medical or Surgical TreatmentДокумент25 страницGastrinomas Medical or Surgical TreatmentTony Miguel Saba SabaОценок пока нет
- Insulin: For Use On The IMMULITE and Immulite 1000 SystemsДокумент27 страницInsulin: For Use On The IMMULITE and Immulite 1000 SystemsnanikhaОценок пока нет
- Hypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Документ12 страницHypoglycemia After Gastric Bypass Surgery. Current Concepts and Controversies 2018Rio RomaОценок пока нет
- HypoglycemiaДокумент68 страницHypoglycemialiaputranti100% (3)
- Clinical Presentation and Diagnostic Approach To Hypoglycemia inДокумент9 страницClinical Presentation and Diagnostic Approach To Hypoglycemia inRichard Loor RomeroОценок пока нет
- Roru Exoendo - PancreasДокумент13 страницRoru Exoendo - PancreasRitz CelsoОценок пока нет
- Insulinoma in A Patient With Type 2 Diabetes: Case Report Nama: Iqbal Putra Amirullah NIM: 030.14.098Документ11 страницInsulinoma in A Patient With Type 2 Diabetes: Case Report Nama: Iqbal Putra Amirullah NIM: 030.14.098desmawitaОценок пока нет
- Insulinoma Case StudyДокумент6 страницInsulinoma Case StudyRanjith RavellaОценок пока нет