Вам также может понравиться
- Hemodialysis, Phosphorus and Calcium, Peritoneal DialysisДокумент29 страницHemodialysis, Phosphorus and Calcium, Peritoneal DialysisTrizha MaeОценок пока нет
- Fundamentals of DialysisДокумент38 страницFundamentals of DialysisGede Purnawinadi100% (1)
- Intradialytic ComplicationsДокумент5 страницIntradialytic Complicationskane1978Оценок пока нет
- Myths of DialysisДокумент26 страницMyths of DialysisSijo Muthukad M100% (1)
- Dialysis DocumentДокумент3 страницыDialysis DocumentLucelle ArellanoОценок пока нет
- Hemodialysi S: Ariane Jake C. Fernandez, RN, MSNДокумент37 страницHemodialysi S: Ariane Jake C. Fernandez, RN, MSNMicah Alexis Candelario100% (3)
- DialysisДокумент34 страницыDialysisdaisy100% (2)
- TypesДокумент3 страницыTypesProser Faith TabaculdeОценок пока нет
- Core Curriculum For The Dialysis Nurse - Module 1Документ7 страницCore Curriculum For The Dialysis Nurse - Module 1green_archerОценок пока нет
- Peritoneal DialysisДокумент23 страницыPeritoneal Dialysismakyofrancis20Оценок пока нет
- Complications Dialysis 12 09Документ47 страницComplications Dialysis 12 09irish_meg316557100% (2)
- Dialysis PresentationДокумент21 страницаDialysis PresentationRon Anderson100% (1)
- Dialysis ExamДокумент10 страницDialysis ExamEljhae AquinoОценок пока нет
- 2013 Dialysis Tech Study Guide PDFДокумент2 страницы2013 Dialysis Tech Study Guide PDFZH. omg sarОценок пока нет
- Renal Replacement Therapies Hemodialysis and Peritoneal DialysisДокумент86 страницRenal Replacement Therapies Hemodialysis and Peritoneal DialysisSabita Tripathi100% (2)
- DIALYSIS ReportingДокумент10 страницDIALYSIS ReportingGlenelyn Grace InfanteОценок пока нет
- HemodialysisДокумент28 страницHemodialysischarlenetan18100% (6)
- DIALYSISДокумент6 страницDIALYSISJobelle AcenaОценок пока нет
- Nephro - CVC Tip SheetДокумент6 страницNephro - CVC Tip Sheetsam m0% (1)
- Hemodialysis and Peritoneal DialysisДокумент57 страницHemodialysis and Peritoneal Dialysisirene joy91% (11)
- Hemodialysis 1Документ25 страницHemodialysis 1Jasmine KaurОценок пока нет
- DIALYSISДокумент30 страницDIALYSISHecel Olita75% (4)
- HemodialysisДокумент9 страницHemodialysisKristine Artes Aguilar100% (2)
- DACUM Competency Profile For Hemodialysis TechnicianДокумент5 страницDACUM Competency Profile For Hemodialysis Technicianmanishbabu100% (1)
- HemodialysisДокумент120 страницHemodialysissigmundmaharajanОценок пока нет
- Complication of Hemodialysis and Their ManagementДокумент52 страницыComplication of Hemodialysis and Their ManagementRetno SumaraОценок пока нет
- Dialysis: Cresencio C. Cajigal, Jr. RN, ManДокумент32 страницыDialysis: Cresencio C. Cajigal, Jr. RN, ManMary Jane Avila Bacquial100% (7)
- Dialysis: Edna Co RN ManДокумент37 страницDialysis: Edna Co RN ManMary Shine GonidaОценок пока нет
- Peritoneal DialysisДокумент17 страницPeritoneal DialysisIan Benedict GuerreroОценок пока нет
- DialysisДокумент34 страницыDialysisAntonio Junior CastroОценок пока нет
- Renal NursinglДокумент36 страницRenal NursinglgireeshsachinОценок пока нет
- Prepared By, Gayathri R 2 Yr MSC (N) UconДокумент41 страницаPrepared By, Gayathri R 2 Yr MSC (N) UconGayathri RОценок пока нет
- Peritoneal DialysisДокумент3 страницыPeritoneal DialysisRovefrances ErpeluaОценок пока нет
- Dialysis Notes 1Документ3 страницыDialysis Notes 1SarahSigrid88% (24)
- Peritoneal DialysisДокумент5 страницPeritoneal DialysisJulienne Sanchez-SalazarОценок пока нет
- DialysisДокумент19 страницDialysisSachin Singh100% (2)
- HemodialysisДокумент13 страницHemodialysisEthel Gretchen Casalla100% (2)
- HemodialysisДокумент22 страницыHemodialysisAlyssa Agravante100% (3)
- Guidebook Kidney DialysisДокумент88 страницGuidebook Kidney Dialysisunfriendly.gy2268Оценок пока нет
- DIALYSISДокумент7 страницDIALYSISIvy E. LantapeОценок пока нет
- Complications of DialysisДокумент7 страницComplications of DialysisDilessandro PieroОценок пока нет
- Certified Hemodialysis Technician ExamДокумент5 страницCertified Hemodialysis Technician Examjohnsonkkuriakose100% (1)
- Peritoneal DialysisДокумент56 страницPeritoneal DialysisVanet100% (1)
- Dialysis PrescriptionДокумент23 страницыDialysis PrescriptionMercy Juliana Jacqualine100% (1)
- DIALYSIS ProcedureДокумент8 страницDIALYSIS ProcedureRaman SamraoОценок пока нет
- End-Stage Renal Disease: An Integrated ApproachОт EverandEnd-Stage Renal Disease: An Integrated ApproachWilliam J. StoneОценок пока нет
- Complications of Hemodialysis and Their Management For NursingДокумент10 страницComplications of Hemodialysis and Their Management For Nursingroserem2000100% (1)
- Renal Replacement TherapyДокумент50 страницRenal Replacement TherapyMalueth Angui100% (1)
- Assignment On DislysisДокумент10 страницAssignment On DislysisSanhati Ghosh Banerjee100% (1)
- Dialysis Basics: DR - Ashutosh Ojha MD, DNB (Gen Med) PDCC-Nephro (Student) GMCH..GuwahatiДокумент36 страницDialysis Basics: DR - Ashutosh Ojha MD, DNB (Gen Med) PDCC-Nephro (Student) GMCH..GuwahatiManish Arya JaiswalОценок пока нет
- Peritoneal DialysisДокумент37 страницPeritoneal Dialysisger668Оценок пока нет
- Peritoneal DialysisДокумент5 страницPeritoneal DialysisLisette TupasОценок пока нет
- Hemodialysis Catheter InfectionДокумент38 страницHemodialysis Catheter InfectionKavidu KeshanОценок пока нет
- Complications of DialysisДокумент26 страницComplications of DialysisrlinaoОценок пока нет
- Dialysis: Notes MS Vol. 2 Krizza Myrrh Gomera Balcita, RNДокумент52 страницыDialysis: Notes MS Vol. 2 Krizza Myrrh Gomera Balcita, RNWhimsey CipresОценок пока нет
- Hemodialysis: Navigation SearchДокумент14 страницHemodialysis: Navigation SearchepingОценок пока нет
- Haemodialysis in ChildrenДокумент38 страницHaemodialysis in ChildrenValliammalShanmugam75% (8)
- HEMODIALYSISДокумент7 страницHEMODIALYSISClarisse ReyesОценок пока нет
- Heat EmergenciesДокумент4 страницыHeat EmergenciesMJ AmarilloОценок пока нет
- Newborn AssessmentДокумент7 страницNewborn AssessmentMJ Amarillo100% (6)
- Pathophysiology DMДокумент1 страницаPathophysiology DMMJ AmarilloОценок пока нет
- Essential Newborn CareДокумент1 страницаEssential Newborn CareMJ AmarilloОценок пока нет
- Casestudy DengueДокумент57 страницCasestudy DengueMJ Amarillo93% (14)
- Casestudy OsteomyelitisДокумент52 страницыCasestudy OsteomyelitisMJ Amarillo84% (19)
- Casestudy Gastric CarcinomaДокумент56 страницCasestudy Gastric CarcinomaMJ Amarillo92% (12)
- HivДокумент26 страницHivMJ AmarilloОценок пока нет
- Orthopedic NursingДокумент202 страницыOrthopedic NursingRigo76801100% (3)
- Presentation (Jessa Urriza)Документ33 страницыPresentation (Jessa Urriza)MJ AmarilloОценок пока нет
- Pathohysiology of Ectopic PregnancyДокумент1 страницаPathohysiology of Ectopic PregnancyMJ AmarilloОценок пока нет
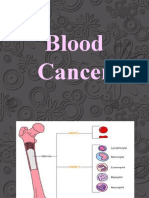
- Blood CancerДокумент34 страницыBlood CancerMJ AmarilloОценок пока нет
- Amniiotic Band Syndrome Cleft Lip/palate Congenital Limb Defects Duodenal AtresiaДокумент18 страницAmniiotic Band Syndrome Cleft Lip/palate Congenital Limb Defects Duodenal AtresiaMJ Amarillo100% (3)
- Chapter 7-Paris To BerlinДокумент20 страницChapter 7-Paris To BerlinMJ Amarillo60% (10)
- Bi-Preterax Slide Set CI 15 - 16Документ35 страницBi-Preterax Slide Set CI 15 - 16drnasim20088171Оценок пока нет
- ONLY WATCH 6th Edition 2015Документ126 страницONLY WATCH 6th Edition 2015Thimios KoukОценок пока нет
- Group Imago and The Stages of Group DevelopmentДокумент16 страницGroup Imago and The Stages of Group DevelopmentNarcis Nagy100% (3)
- Metabolite KineticsДокумент41 страницаMetabolite KineticsZacharielОценок пока нет
- Narrative Therapy Tree of Life ProjectДокумент2 страницыNarrative Therapy Tree of Life ProjecttduongОценок пока нет
- Philosophy Palliative Care and End of Life Care Per 15-02-2021Документ33 страницыPhilosophy Palliative Care and End of Life Care Per 15-02-2021rizki ikhsanОценок пока нет
- Post Traumatic Stress Disorder PTSD As An Over Activation of Sympathetic Nervous System An Alternative View 2167 1222.1000181Документ3 страницыPost Traumatic Stress Disorder PTSD As An Over Activation of Sympathetic Nervous System An Alternative View 2167 1222.1000181Andi ANDIKAОценок пока нет
- BHU Daily Stock PerformaДокумент6 страницBHU Daily Stock PerformabilalОценок пока нет
- BARC TrainingДокумент6 страницBARC Trainingashfaqk100% (1)
- CalgaryДокумент44 страницыCalgaryGifuGifuОценок пока нет
- A Re-Evaluation of Acting Out in Relation To Working ThroughДокумент11 страницA Re-Evaluation of Acting Out in Relation To Working ThroughUriel García VarelaОценок пока нет
- Healthy Food PDFДокумент8 страницHealthy Food PDFnurul syafizatul shahirahОценок пока нет
- Post Operative and Pre Prosthetic ManagementДокумент38 страницPost Operative and Pre Prosthetic ManagementTanzeelah RajawОценок пока нет
- NSAID Safety Audit Jan2019 Vs6Документ10 страницNSAID Safety Audit Jan2019 Vs6Shokooh MansouriОценок пока нет
- Jethani 2022Документ3 страницыJethani 2022febyolaОценок пока нет
- Chap.30 Complications From Heart Disease WordДокумент6 страницChap.30 Complications From Heart Disease WordcaisakiОценок пока нет
- Clinical Massage Therapy - S. Jurch Hill, 2009) WWДокумент562 страницыClinical Massage Therapy - S. Jurch Hill, 2009) WWMohsen Bt92% (12)
- Powerpoint Template FinalДокумент53 страницыPowerpoint Template Finalapi-265054719Оценок пока нет
- CPAP SlidesДокумент52 страницыCPAP SlidesAnusha Verghese100% (1)
- FNCPДокумент2 страницыFNCPJerecho Ramon R. ArciagaОценок пока нет
- Vertigo Vertigoheel 2001Документ7 страницVertigo Vertigoheel 2001Dr. Nancy Malik100% (1)
- Art Therapy and Dialectical Behavioral Therapy - A WorkbookДокумент35 страницArt Therapy and Dialectical Behavioral Therapy - A WorkbookZainab BorjiОценок пока нет
- M1 Introduction To Manual TherapyДокумент101 страницаM1 Introduction To Manual TherapySylvia LoongОценок пока нет
- Rubella: Congenital Clinically Significant Congenital MalformationsДокумент8 страницRubella: Congenital Clinically Significant Congenital MalformationsAlexandraОценок пока нет
- Glimpse of My ResearchДокумент4 страницыGlimpse of My Researchमनोज जैनОценок пока нет
- Nutrition AssessmentДокумент11 страницNutrition Assessmentnikhild77Оценок пока нет
- Master Kinesiotaping HandoutДокумент11 страницMaster Kinesiotaping HandoutcosasdeangelОценок пока нет
- 2 CP Bekam Angin Tahap 3Документ8 страниц2 CP Bekam Angin Tahap 3Norhissam MustafaОценок пока нет
- Decreasing Lithium PrescriptionsДокумент5 страницDecreasing Lithium PrescriptionsJeffrey FawcettОценок пока нет
- Gross Motor Development 6to12yearsДокумент17 страницGross Motor Development 6to12yearsGul RockzzОценок пока нет