Вам также может понравиться
- 93 - Operating Room ProtocolДокумент25 страниц93 - Operating Room ProtocolFelix Kwenandar100% (1)
- Scott Stewarts Surviving Schizophrenia Story PDFДокумент113 страницScott Stewarts Surviving Schizophrenia Story PDFscott stewartОценок пока нет
- Battery Exam 2017 Level 4Документ202 страницыBattery Exam 2017 Level 4Mevelle Laranjo AsuncionОценок пока нет
- NABHДокумент12 страницNABHGirish GVОценок пока нет
- NABH DocДокумент12 страницNABH DocYoutube premiumОценок пока нет
- Final Pre Accreditation Entry Level Standards For Hospital Book PDFДокумент53 страницыFinal Pre Accreditation Entry Level Standards For Hospital Book PDFams_1234100% (1)
- Planning and Management of Clinical Service DepartmentДокумент41 страницаPlanning and Management of Clinical Service DepartmentDrPriyanka Prashant PawsheОценок пока нет
- People Management in Hospitat IndustryДокумент29 страницPeople Management in Hospitat Industrychintamani_krishnaОценок пока нет
- Question Bank: Paper 3 - Organisation of Hospital ServicesДокумент5 страницQuestion Bank: Paper 3 - Organisation of Hospital ServicesDr. Rakshit SolankiОценок пока нет
- Role & Importance of Medical Records: Mahboob Ali Khan MHA, CPHQ Consultant HealthcareДокумент60 страницRole & Importance of Medical Records: Mahboob Ali Khan MHA, CPHQ Consultant HealthcareDr. Asma QureshiОценок пока нет
- Hospital ManagementДокумент29 страницHospital ManagementRohit YadavОценок пока нет
- Admitting Dept PlanningДокумент22 страницыAdmitting Dept PlanningPrasannaa VijayaranganОценок пока нет
- ICAP Basic ICRA With MatrixДокумент4 страницыICAP Basic ICRA With MatrixmiptahulОценок пока нет
- Job Responsibilities FoДокумент4 страницыJob Responsibilities FoKumar BalramОценок пока нет
- Hospital Management SystemДокумент3 страницыHospital Management SystemRida beygОценок пока нет
- 100 Bedded Hospital LectureДокумент53 страницы100 Bedded Hospital LectureIngyin KhinОценок пока нет
- Define Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalДокумент15 страницDefine Medical Audit. Describe The Conditions, Prerequisites & Steps For Conducting Medical Audit in A General HospitalAbdul RahamanОценок пока нет
- Challenges NabhДокумент24 страницыChallenges NabhEka BОценок пока нет
- Advence Hospital Management System PDFДокумент6 страницAdvence Hospital Management System PDFMd Nazmul IslamОценок пока нет
- NABH Assessment - Institutional Ethics CommitteesДокумент4 страницыNABH Assessment - Institutional Ethics CommitteesAmitKumarОценок пока нет
- NABH IntroductionДокумент12 страницNABH IntroductionKrishna100% (1)
- Drugs Commonly Available in The Critical Care UnitДокумент10 страницDrugs Commonly Available in The Critical Care UnitEggy PascualОценок пока нет
- Checklist of Pathology Laboratory and Its Quality Indicators For NABH Accreditation PreparationДокумент3 страницыChecklist of Pathology Laboratory and Its Quality Indicators For NABH Accreditation PreparationPayal Thakker100% (1)
- Hospital DepartmentsДокумент16 страницHospital DepartmentsfictoriaОценок пока нет
- Crash Cart Policy and Checklist in HospitalДокумент7 страницCrash Cart Policy and Checklist in HospitalDnyanesh AitalwadОценок пока нет
- Hospital Management SystemДокумент23 страницыHospital Management SystemBlndОценок пока нет
- Different Departments Required in A HospitalДокумент11 страницDifferent Departments Required in A HospitalEdsel Dudes AbanteОценок пока нет
- Clinical Casuality ManagementДокумент6 страницClinical Casuality ManagementswathiprasadОценок пока нет
- Activities Patient SafetyДокумент13 страницActivities Patient SafetyummuawisyОценок пока нет
- How To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairДокумент9 страницHow To Move The Patient From The Bed To The Wheelchair How To Move The Patient From The Bed To The WheelchairAfniy ApriliaОценок пока нет
- IPSG PresentationДокумент38 страницIPSG Presentationmuhammed shamaa100% (1)
- Endoscopy Unit Resources - Users Guide To Achieving A JAG Compliant Endoscopy EnvironmentДокумент21 страницаEndoscopy Unit Resources - Users Guide To Achieving A JAG Compliant Endoscopy Environmentmonir61Оценок пока нет
- NABH IntroductionДокумент9 страницNABH IntroductionKrishnaОценок пока нет
- Evaluation of Outpatient Department in A Public Super Speciality Hospital in IndiaДокумент4 страницыEvaluation of Outpatient Department in A Public Super Speciality Hospital in IndiaMadhusudan MОценок пока нет
- Clarification On Fire SafetyДокумент1 страницаClarification On Fire SafetyNaviin KrishnanОценок пока нет
- JCI Accreditation Presentation 4Документ53 страницыJCI Accreditation Presentation 4Osama MarzoukОценок пока нет
- 2011 Newborn Care SOP 29-11-11Документ95 страниц2011 Newborn Care SOP 29-11-11Safiqul Islam ShawnОценок пока нет
- SWOR Analysis orДокумент4 страницыSWOR Analysis orNoel Telosa0% (1)
- 5 Reducing Time To Analgesia in The Emergency Department Using AДокумент10 страниц5 Reducing Time To Analgesia in The Emergency Department Using AMegaHandayaniОценок пока нет
- Informed ConsentДокумент17 страницInformed ConsentKenvyne Quides-CalugayОценок пока нет
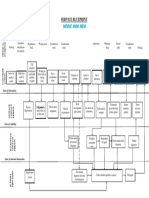
- Service Blueprint Medical CenterДокумент1 страницаService Blueprint Medical CenterNguyen Le Hoang KimОценок пока нет
- Endoscopy UnitДокумент77 страницEndoscopy Unitmonir6150% (2)
- Assessment and Re-Assessment of Patients According To The Scope of ServiceДокумент9 страницAssessment and Re-Assessment of Patients According To The Scope of Servicegiya nursingОценок пока нет
- Cardiac Cath Lab - An OverviewДокумент21 страницаCardiac Cath Lab - An OverviewPravallika ReddyОценок пока нет
- Hospital Antibiotic PolicyДокумент5 страницHospital Antibiotic PolicyNaveen ArichwalОценок пока нет
- Quality Manager Job Description - 09-13Документ3 страницыQuality Manager Job Description - 09-13DrSaswat LincolnОценок пока нет
- Health Records: Organization and Management of Medical Record DepartmentДокумент24 страницыHealth Records: Organization and Management of Medical Record Departmentosama rf100% (1)
- MRDДокумент17 страницMRDPrasoon BanerjeeОценок пока нет
- Master in Hospital MGT - SyllabusДокумент65 страницMaster in Hospital MGT - SyllabusArpit Gupta100% (1)
- Hourly Round ProjectДокумент8 страницHourly Round ProjectaustinisaacОценок пока нет
- NABH Quality ConnectДокумент16 страницNABH Quality ConnectNeeraj JoshiОценок пока нет
- GOC - Rates - July 2019 - CompleteДокумент6 страницGOC - Rates - July 2019 - CompleteAkbar ShaikОценок пока нет
- Central Triage ProtocolДокумент1 страницаCentral Triage Protocolgechworkneh38Оценок пока нет
- HmisДокумент14 страницHmis166873100% (1)
- 4+Roadmap+to+NABH+ +finalДокумент18 страниц4+Roadmap+to+NABH+ +finalSameer BugdeОценок пока нет
- Apex Manual RPOCДокумент70 страницApex Manual RPOCtanisha100% (1)
- National Board of Examinations Revised Curriculum For Competency Based Training of DNB CandidatesДокумент48 страницNational Board of Examinations Revised Curriculum For Competency Based Training of DNB CandidatestejluОценок пока нет
- KPI Discussion Paper 3Документ22 страницыKPI Discussion Paper 3Manager HR Hijaz Hospital100% (1)
- Arero Primary Hospital Triage ProtocolДокумент4 страницыArero Primary Hospital Triage Protocolsami ketemaОценок пока нет
- Guidelines For SB and U5 Mortality Reporting System 2nd Edition 2018Документ24 страницыGuidelines For SB and U5 Mortality Reporting System 2nd Edition 2018Roziha RahimОценок пока нет
- Guidebook Hope PDFДокумент34 страницыGuidebook Hope PDFDr MukeshОценок пока нет
- September 2015 Ophthalmic PearlsДокумент3 страницыSeptember 2015 Ophthalmic PearlsLouis WakumОценок пока нет
- Midwifery Practice at The Massachusetts General Hospital Vincent Obstetrics andДокумент1 страницаMidwifery Practice at The Massachusetts General Hospital Vincent Obstetrics andapi-20955008Оценок пока нет
- Vitamin C Pamphlet PDFДокумент2 страницыVitamin C Pamphlet PDFgreeenbee100% (2)
- Chromosome 19Документ12 страницChromosome 19Neil Justin BermoyОценок пока нет
- FNCP FormatДокумент12 страницFNCP FormatChristi MilanОценок пока нет
- Kavita Priya Labetalol in Pih - IДокумент58 страницKavita Priya Labetalol in Pih - IKavita PriyaОценок пока нет
- Nursing Care Plan: Ha Noi Medical UniversityДокумент17 страницNursing Care Plan: Ha Noi Medical UniversityThảo LÊОценок пока нет
- Bipolar Disorder or ManicДокумент16 страницBipolar Disorder or Manicbbkanil100% (1)
- Therapeutic ExercisesДокумент50 страницTherapeutic ExercisesBalram Jha100% (3)
- Post-Mortem ExaminationДокумент7 страницPost-Mortem ExaminationLeninRickyОценок пока нет
- Icon Strategies and Quality PracticeДокумент4 страницыIcon Strategies and Quality PracticeSammy ChegeОценок пока нет
- Acute Respiratory Failure: Part 1. Failure in OxygenationДокумент6 страницAcute Respiratory Failure: Part 1. Failure in OxygenationnytenurseОценок пока нет
- Concept of Health Disease and PreventionДокумент33 страницыConcept of Health Disease and PreventionitdocОценок пока нет
- Seinfeld Syncope'': To The EditorДокумент1 страницаSeinfeld Syncope'': To The EditorJason ChambersОценок пока нет
- VISION 2020 Priority Eye DiseasesДокумент7 страницVISION 2020 Priority Eye DiseaseschandradwtrОценок пока нет
- What Is HyperthymesiaДокумент2 страницыWhat Is HyperthymesiaCarlos BellatinОценок пока нет
- Swashbuckler Approach and Surgical Technique in Severely Comminuted Fractures of The Distal FemurДокумент8 страницSwashbuckler Approach and Surgical Technique in Severely Comminuted Fractures of The Distal FemurPramod Nk100% (2)
- 10 Rights in Drug AdministrationДокумент25 страниц10 Rights in Drug AdministrationNathaniel PulidoОценок пока нет
- Colour BlindnessДокумент4 страницыColour BlindnessDanial HazimОценок пока нет
- Vitamin K Administration in The Newborn GuidelineДокумент10 страницVitamin K Administration in The Newborn GuidelineAna Sarah KurniaОценок пока нет
- Cardiovascular Disorders ExamДокумент13 страницCardiovascular Disorders ExambobtagubaОценок пока нет
- Branchial Cleft CystДокумент4 страницыBranchial Cleft CystCharmila SariОценок пока нет
- Atropine Sulfate Drug STudyДокумент2 страницыAtropine Sulfate Drug STudyLiway100% (1)
- Urinary CathetersДокумент5 страницUrinary CathetersJyoti Pariyar100% (1)
- Bianchi Czerwinski DIVA 2011-11-14Документ10 страницBianchi Czerwinski DIVA 2011-11-14Negreanu AncaОценок пока нет
- Erythema Nodosum LeprosumДокумент23 страницыErythema Nodosum LeprosumSulfia SuhardiОценок пока нет
- 3003 - Position Description-Performance Evaluation - Dialysis Services Medical DirectorДокумент8 страниц3003 - Position Description-Performance Evaluation - Dialysis Services Medical DirectorPriambadaPutraОценок пока нет
- Methamphetamine 10Документ4 страницыMethamphetamine 10Teodora NeshovaОценок пока нет