Вам также может понравиться
- DELIRIUM PresentationДокумент26 страницDELIRIUM PresentationAnkush Sharma100% (1)
- Etiopathogenesis of DeliriumДокумент36 страницEtiopathogenesis of DeliriumAarti Gupta100% (1)
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesОт EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesРейтинг: 5 из 5 звезд5/5 (1)
- Delirium: EpidemiologyДокумент8 страницDelirium: EpidemiologyNunuОценок пока нет
- Schizophrenia OverviewДокумент8 страницSchizophrenia OverviewRiscky LauwОценок пока нет
- Classification of Psychiatric Disorders by Dr. FatimaДокумент12 страницClassification of Psychiatric Disorders by Dr. FatimaRahul Kumar Diwakar100% (1)
- DEMENTIAДокумент42 страницыDEMENTIAputri maharaniОценок пока нет
- Psychiatric EmergenciesДокумент27 страницPsychiatric EmergenciesshahiraazОценок пока нет
- Delusional DisorderДокумент12 страницDelusional Disorderapi-3797941100% (2)
- Geriatric Psychiatry LectureДокумент113 страницGeriatric Psychiatry LectureabrihamОценок пока нет
- Depression Interview QuestionsДокумент3 страницыDepression Interview QuestionsStarlin Vijay Mythri100% (1)
- Lithium ToxicityДокумент9 страницLithium Toxicityrajeshisaac100% (2)
- DeliriumДокумент2 страницыDeliriumAngelique van Tonder100% (2)
- Chapter 7 Study GuideДокумент4 страницыChapter 7 Study GuidejbradeeОценок пока нет
- Se 04 Abpsych PDFДокумент27 страницSe 04 Abpsych PDFBea SengcoОценок пока нет
- Mental Status EvaluationДокумент7 страницMental Status Evaluationmunir houseОценок пока нет
- EATING DISORDERS: Note Taking OutlineДокумент6 страницEATING DISORDERS: Note Taking OutlinePaula GarciaОценок пока нет
- Huntington's Disease: A Clinical ReviewДокумент8 страницHuntington's Disease: A Clinical ReviewAlba RОценок пока нет
- Introduction To Psychiatric NursingДокумент11 страницIntroduction To Psychiatric NursingjoycechicagoОценок пока нет
- Mental Health E3 QuizletДокумент2 страницыMental Health E3 QuizletTodd ColeОценок пока нет
- Psychiatric Mental Health Nursing PresentationДокумент28 страницPsychiatric Mental Health Nursing PresentationDanics de LeonОценок пока нет
- Neurobiology and BehaviorДокумент24 страницыNeurobiology and BehaviorNaveen Eldose100% (1)
- Geriatric Giants - DR SeymourДокумент108 страницGeriatric Giants - DR SeymourSharon Mallia100% (1)
- PsychopharmacologyДокумент32 страницыPsychopharmacologyCms CSU100% (1)
- DeliriumДокумент1 страницаDeliriumAlex Peng100% (1)
- Acute Psychotic DisordersДокумент70 страницAcute Psychotic DisordersDenso Antonius LimОценок пока нет
- Case Vignette. EpilepsyДокумент8 страницCase Vignette. EpilepsyAizel ManiagoОценок пока нет
- Joshua Dodot Case StudyДокумент2 страницыJoshua Dodot Case StudyJoshua Ringor100% (1)
- Nursing Process in Psychiatric Unit - 3Документ138 страницNursing Process in Psychiatric Unit - 3Lina DsouzaОценок пока нет
- Nicotine Related DisordersДокумент74 страницыNicotine Related DisordersKuldeep singhОценок пока нет
- Mental Health TipsДокумент10 страницMental Health Tipsnicki scheffler100% (2)
- Nursing Department: Saint Mary's UniversityДокумент6 страницNursing Department: Saint Mary's UniversityCheetah GemmaОценок пока нет
- OCD and Related DisordersДокумент40 страницOCD and Related Disorderscatherine faith gallemitОценок пока нет
- Neurotransmitters in Schizophrenia: Dr. Adel El SheshaiДокумент47 страницNeurotransmitters in Schizophrenia: Dr. Adel El SheshaielvinegunawanОценок пока нет
- Delirium: DR A.Vijaya Chandra Reddy Associate Professor of Psychaitry Dept. of Psychiatry Rims, KadapaДокумент20 страницDelirium: DR A.Vijaya Chandra Reddy Associate Professor of Psychaitry Dept. of Psychiatry Rims, KadapaPraveen Pravii100% (1)
- Function-Memory, Smell And: Persecutory / Paranoid Delusions - Involve TheДокумент4 страницыFunction-Memory, Smell And: Persecutory / Paranoid Delusions - Involve TheMark Christian CaasiОценок пока нет
- Common Psychiatric DisordersДокумент3 страницыCommon Psychiatric DisordersWaheedullah AhmadiОценок пока нет
- Bipolar Disorder: Presented By: Group 2Документ19 страницBipolar Disorder: Presented By: Group 2Pao DelossantosОценок пока нет
- Anxiety and Stress-Related DisordersДокумент26 страницAnxiety and Stress-Related Disordersunpredictable_stoneОценок пока нет
- Mental Health Nursing - WK 1Документ10 страницMental Health Nursing - WK 1Chalcey PolsonОценок пока нет
- Lithium Monitoring and ToxicityДокумент22 страницыLithium Monitoring and ToxicityLindaОценок пока нет
- 2b - Personality DisordersДокумент27 страниц2b - Personality DisordersaldreinОценок пока нет
- Geriatrics 2023 FinalДокумент119 страницGeriatrics 2023 FinalBelinda ELISHAОценок пока нет
- Organic Brain Disorder-1Документ69 страницOrganic Brain Disorder-1Howell MathewОценок пока нет
- Overview of Mood DisordersДокумент6 страницOverview of Mood DisordersMaria Jezabel CaipangОценок пока нет
- Bipolar Disorder PamphletДокумент2 страницыBipolar Disorder Pamphletapi-3134075020% (1)
- Introduction of Psychiatric NursingДокумент26 страницIntroduction of Psychiatric NursingadiОценок пока нет
- Alzheimeru2019s DiseaseДокумент17 страницAlzheimeru2019s Diseaseapi-262538456100% (1)
- Bipolar Disorder PowerpointДокумент30 страницBipolar Disorder PowerpointZara SheikhОценок пока нет
- Disorders RushedДокумент40 страницDisorders Rushedapi-391411195Оценок пока нет
- Dementia: .. (Give The Reason Why)Документ8 страницDementia: .. (Give The Reason Why)KAILISH RHOE PADEROОценок пока нет
- Psychiatry NotesДокумент123 страницыPsychiatry NotesKyoheirwe vanessaОценок пока нет
- PSYCHIATRIC NURSING AnjaliДокумент47 страницPSYCHIATRIC NURSING AnjaliAnjali GuptaОценок пока нет
- Session 7 Psychiatric AssessmentДокумент54 страницыSession 7 Psychiatric AssessmentPetroОценок пока нет
- C-L Psychiatry or Clinical Liaison PsychiatryДокумент15 страницC-L Psychiatry or Clinical Liaison PsychiatryMary Joy Oros-VallejeraОценок пока нет
- Cultural Issue Schizophrenia IndiaДокумент58 страницCultural Issue Schizophrenia IndiaSam InvincibleОценок пока нет
- SchizophreniaДокумент58 страницSchizophreniaArpit AroraОценок пока нет
- Hallucination, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОт EverandHallucination, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsОценок пока нет
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeОт EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeОценок пока нет
- Article Beginning New Generation 6-Cylinder N52Документ73 страницыArticle Beginning New Generation 6-Cylinder N52Sabry NadourОценок пока нет
- DIP3E Chapter02 ArtДокумент57 страницDIP3E Chapter02 ArtShahid MehmoodОценок пока нет
- Amg Remove - Install Camshaft AdjustersДокумент5 страницAmg Remove - Install Camshaft AdjustersRoland HendriksОценок пока нет
- T-119C T-243 T-206ELG: 3 Prong Case Opener Movement Holder Brass Suitable For Ladies and Gents Movements Screwdriver SetДокумент2 страницыT-119C T-243 T-206ELG: 3 Prong Case Opener Movement Holder Brass Suitable For Ladies and Gents Movements Screwdriver Setblackarrow1990Оценок пока нет
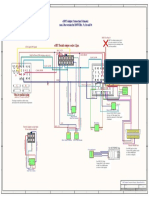
- eNBT Adapter (Non I-Bus) Wiring DiagramДокумент1 страницаeNBT Adapter (Non I-Bus) Wiring Diagramdcde2004Оценок пока нет
- DIY Retrofit Folding Mirrors E88Документ9 страницDIY Retrofit Folding Mirrors E88dcde2004Оценок пока нет
- 2015 Anatomy 2 Review ListДокумент4 страницы2015 Anatomy 2 Review Listdcde2004Оценок пока нет
- Some Things To Think About Before Considering SingaporeДокумент1 страницаSome Things To Think About Before Considering Singaporedcde2004Оценок пока нет
- BMW Code SheetДокумент338 страницBMW Code SheetAleksey Lakomov76% (29)
- T-119C T-243 T-206ELG: 3 Prong Case Opener Movement Holder Brass Suitable For Ladies and Gents Movements Screwdriver SetДокумент2 страницыT-119C T-243 T-206ELG: 3 Prong Case Opener Movement Holder Brass Suitable For Ladies and Gents Movements Screwdriver Setblackarrow1990Оценок пока нет
- Functional Module ErrorДокумент2 страницыFunctional Module Errordcde2004Оценок пока нет
- Custom ShopДокумент10 страницCustom Shopdcde2004100% (1)
- 3 Way StreetДокумент12 страниц3 Way Streetdcde2004Оценок пока нет
- Some Things To Think About Before Considering SingaporeДокумент10 страницSome Things To Think About Before Considering Singaporedcde2004Оценок пока нет
- Tong Hua (Fairy Tale) - by Guang Liang (Piano)Документ3 страницыTong Hua (Fairy Tale) - by Guang Liang (Piano)Mitchell Yum50% (2)
- Green Antigen PresentationДокумент25 страницGreen Antigen Presentationdcde2004Оценок пока нет
- Mahou No Kotoba (Instrumental) PDFДокумент12 страницMahou No Kotoba (Instrumental) PDFdcde2004Оценок пока нет
- Pure Mixed and Entangled StatesДокумент27 страницPure Mixed and Entangled Statesdcde2004Оценок пока нет
- Some Things To Think About Before Considering SingaporeДокумент10 страницSome Things To Think About Before Considering Singaporedcde2004Оценок пока нет
- 2 Level Atom EasyДокумент10 страниц2 Level Atom Easydcde2004Оценок пока нет
- J35 - Inlay LayoutДокумент1 страницаJ35 - Inlay Layoutdcde2004Оценок пока нет
- Final Material MicroДокумент89 страницFinal Material Microdcde2004Оценок пока нет
- Oshio DДокумент3 страницыOshio Ddcde2004Оценок пока нет
- Church Worship SongsДокумент5 страницChurch Worship Songsdcde2004Оценок пока нет
- If I Ain T Got You Piano Accompaniment Alicia KeysДокумент4 страницыIf I Ain T Got You Piano Accompaniment Alicia Keysdcde2004Оценок пока нет
- Wind Song Kotaro OshioДокумент3 страницыWind Song Kotaro Oshiodcde2004100% (1)
- CH01 Tute AnswersДокумент8 страницCH01 Tute Answersdcde2004100% (1)
- Magic Wave July 2011 PDF 69Документ19 страницMagic Wave July 2011 PDF 69Budi TurmokoОценок пока нет
- Long Term Care ServicesДокумент8 страницLong Term Care ServicesCole GoОценок пока нет
- Cardiovascular System - Heart IntroДокумент6 страницCardiovascular System - Heart IntroKate Angeline TanОценок пока нет
- Conduction System of HeartДокумент2 страницыConduction System of HeartEINSTEIN2DОценок пока нет
- Nephrotic Case Study With AnswersДокумент3 страницыNephrotic Case Study With AnswersKBОценок пока нет
- Betnovate NДокумент11 страницBetnovate NAhmed KhanОценок пока нет
- Drug Interaction Report PDFДокумент111 страницDrug Interaction Report PDFbaerbaОценок пока нет
- Nipa Virus InfectionsДокумент83 страницыNipa Virus Infectionsanon_547200245Оценок пока нет
- Itch in Elderly People: A Cross-Sectional Study: Investigative ReportДокумент9 страницItch in Elderly People: A Cross-Sectional Study: Investigative ReportPatricia JesikaОценок пока нет
- Reduction in Left Ventricular Hypertrophy in Hypertensive Patients Treated With Enalapril, Losartan or The Combination of Enalapril and LosartanДокумент7 страницReduction in Left Ventricular Hypertrophy in Hypertensive Patients Treated With Enalapril, Losartan or The Combination of Enalapril and LosartanDiana De La CruzОценок пока нет
- PericarditisДокумент3 страницыPericarditisKhalid Mahmud Arifin0% (1)
- Acute GastroenteritisДокумент8 страницAcute Gastroenteritisleizel_seranОценок пока нет
- Renal Cell Carcinoma Tuberous SclerosisДокумент48 страницRenal Cell Carcinoma Tuberous SclerosisPiyushОценок пока нет
- CHAPTER 7 Miscellaneous ProtozoaДокумент4 страницыCHAPTER 7 Miscellaneous ProtozoaTawfeeq AuqbiОценок пока нет
- Urolithiasis NP: Deficit of KnowledgeДокумент2 страницыUrolithiasis NP: Deficit of Knowledgevictor zhefaОценок пока нет
- Covid Report: Mr. Rakesh SharmaДокумент1 страницаCovid Report: Mr. Rakesh Sharmavishal sharmaОценок пока нет
- Encefalitis LimbicaДокумент11 страницEncefalitis LimbicaRandy UlloaОценок пока нет
- Surgical Group - Normal Physiologic Changes in Aging Affecting Various SystemsДокумент20 страницSurgical Group - Normal Physiologic Changes in Aging Affecting Various SystemsKyra Bianca R. FamacionОценок пока нет
- Session 17 Cfu PDFДокумент1 страницаSession 17 Cfu PDFFelecity Del Valle PaduaОценок пока нет
- 0.3 MG 3 Times A Day HairДокумент6 страниц0.3 MG 3 Times A Day Hairlakshay kumarОценок пока нет
- Journal of The ACP in Womens HealthДокумент108 страницJournal of The ACP in Womens HealthRobert SandeepОценок пока нет
- Ncma 219 Finals CompleteДокумент70 страницNcma 219 Finals CompleteKENSEY MOORE EBROLEОценок пока нет
- Effect of Sun - Venus Sharing Same HouseДокумент5 страницEffect of Sun - Venus Sharing Same Housearunprasath1978100% (1)
- TestДокумент2 страницыTestSuperTotie LandritoОценок пока нет
- Medical Surgical NursingДокумент110 страницMedical Surgical Nursingarjetahoward100% (5)
- FY13 April Epilepsy Pamphlet PDFДокумент2 страницыFY13 April Epilepsy Pamphlet PDFLeo HurtadoОценок пока нет
- ProtozoaДокумент132 страницыProtozoaAb AbОценок пока нет
- Differential Diagnosis in Dermatology Fourth Edition: Richard Ashton, Barbara Leppard and Hywel CooperДокумент30 страницDifferential Diagnosis in Dermatology Fourth Edition: Richard Ashton, Barbara Leppard and Hywel CooperAussie Aulia100% (1)
- Mild Diabetic Ketoacidosis2Документ10 страницMild Diabetic Ketoacidosis2GorgieОценок пока нет
- Is Agt The New Gene For Muscle Performance An Analysis of Agt Actn3 Ppara and Igf2 On Athletic Performance Muscle Size and Body Fa Z1yrДокумент6 страницIs Agt The New Gene For Muscle Performance An Analysis of Agt Actn3 Ppara and Igf2 On Athletic Performance Muscle Size and Body Fa Z1yrLeticia GasparОценок пока нет