Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Reader's Digest January 2013Документ148 страницReader's Digest January 2013pereira_jus3430Оценок пока нет
- Lymphoid Leukemia in DogsДокумент15 страницLymphoid Leukemia in Dogstaner_soysurenОценок пока нет
- Rules and Guidelines For Mortality and Morbidity CodingДокумент5 страницRules and Guidelines For Mortality and Morbidity Codingzulfikar100% (2)
- 1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-ConceptionДокумент2 страницы1.3 Describe Factors That May Impact Upon The Development of The Baby During: Pre-Conceptionjoel TorresОценок пока нет
- Astellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeДокумент3 страницыAstellas Pharma: Launches Irribow OD Tablets in Japan For Diarrhea-Predominant Irritable Bowel SyndromeHerry HendrayadiОценок пока нет
- Practical Guide To Joint and Soft Tissue Injection TechniquesДокумент5 страницPractical Guide To Joint and Soft Tissue Injection TechniquesHerry HendrayadiОценок пока нет
- Lifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingДокумент176 страницLifecycle Management Strategies Maximizing ROI Through Indication Expansion Reformulation and Rx-To-OTC SwitchingHerry Hendrayadi100% (1)
- Anti-Inflammatory Drugs Даша ОкончательнДокумент82 страницыAnti-Inflammatory Drugs Даша ОкончательнHerry HendrayadiОценок пока нет
- Standard Step-Wise Timelines in The Drug Discovery ProcessДокумент19 страницStandard Step-Wise Timelines in The Drug Discovery ProcessHerry HendrayadiОценок пока нет
- The Blockbuster Drugs Outlook PDFДокумент259 страницThe Blockbuster Drugs Outlook PDFHerry HendrayadiОценок пока нет
- Indication Expansion Opportunities For Successful Lifecycle ManagementДокумент144 страницыIndication Expansion Opportunities For Successful Lifecycle ManagementHerry HendrayadiОценок пока нет
- Management Pocketbooks - The Balance Sheet PocketbookДокумент309 страницManagement Pocketbooks - The Balance Sheet PocketbookHerry Hendrayadi100% (1)
- Top 15 Therapeutic 2008 PDFДокумент95 страницTop 15 Therapeutic 2008 PDFHerry HendrayadiОценок пока нет
- Growth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsДокумент176 страницGrowth Strategies in Generics Innovative and Aggressive Strategies and Their Impact On Branded PharmaceuticalsHerry HendrayadiОценок пока нет
- StarWarsInsider February2018 PDFДокумент84 страницыStarWarsInsider February2018 PDFHerry Hendrayadi100% (1)
- Achieving Market Dominance Through ReformulationДокумент223 страницыAchieving Market Dominance Through ReformulationHerry HendrayadiОценок пока нет
- Systemic Lupus Erythematosus and Neuropsychiatric DiseaseДокумент56 страницSystemic Lupus Erythematosus and Neuropsychiatric DiseaseHerry HendrayadiОценок пока нет
- Ijss Aug Oa12Документ5 страницIjss Aug Oa12Herry HendrayadiОценок пока нет
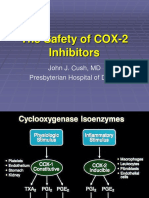
- The Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasДокумент29 страницThe Safety of COX-2 Inhibitors: John J. Cush, MD Presbyterian Hospital of DallasHerry HendrayadiОценок пока нет
- Corticosteroid Present 12-2Документ46 страницCorticosteroid Present 12-2Herry HendrayadiОценок пока нет
- Rheumatology 101:: What You Need To Know For Your Ambulatory Medicine ExperienceДокумент40 страницRheumatology 101:: What You Need To Know For Your Ambulatory Medicine ExperienceHerry HendrayadiОценок пока нет
- Clozapine Therapy Training FINAL 3-10-15Документ23 страницыClozapine Therapy Training FINAL 3-10-15Herry HendrayadiОценок пока нет
- Polymyalgia Rheumatic Symptoms Diagnosis and TreatmentДокумент2 страницыPolymyalgia Rheumatic Symptoms Diagnosis and TreatmentHas SimОценок пока нет
- Oral RevalidaДокумент3 страницыOral RevalidaJaye DangoОценок пока нет
- CSF Catalogue enДокумент76 страницCSF Catalogue enHarshitShuklaОценок пока нет
- Birth Defects and Prenatal DiagnosisДокумент49 страницBirth Defects and Prenatal DiagnosiskurniaОценок пока нет
- Health Talk TopicsДокумент3 страницыHealth Talk Topicsvarshasharma0562% (13)
- Acutrak2 Radial Head Case StudyДокумент2 страницыAcutrak2 Radial Head Case StudyDinesh KumarОценок пока нет
- Actinomycetes Staining MethodsДокумент14 страницActinomycetes Staining MethodsvikasОценок пока нет
- Tips To Increase Speed of AssessmentДокумент6 страницTips To Increase Speed of AssessmentEsmareldah Henry SirueОценок пока нет
- Unit 1 Chap 1 and 2Документ7 страницUnit 1 Chap 1 and 2Ariane Grace OcampoОценок пока нет
- Arnica Montana - FayazuddinДокумент13 страницArnica Montana - FayazuddinMohammad AtaОценок пока нет
- 5th ReflectionДокумент2 страницы5th Reflectionapi-478150357Оценок пока нет
- A Case Study On MalariaДокумент10 страницA Case Study On MalariaAnant KumarОценок пока нет
- Enema Instructional BookletДокумент34 страницыEnema Instructional Bookletmumtean cosminОценок пока нет
- Nasogastric Gastrostomy Tube Feedling Guidelines v1.4Документ45 страницNasogastric Gastrostomy Tube Feedling Guidelines v1.4bandarascbОценок пока нет
- Chapter 29 Practice TestДокумент8 страницChapter 29 Practice Testnursingstudentd100% (1)
- Filtvebis Xelovnuri Ventilaciis Tanamedrove Metodebi Da RejimebiДокумент45 страницFiltvebis Xelovnuri Ventilaciis Tanamedrove Metodebi Da RejimebiMiranda BeridzeОценок пока нет
- 1 - Indications For Removal of TeethДокумент7 страниц1 - Indications For Removal of TeethLama NahedОценок пока нет
- ACPH - Testimonial FormДокумент5 страницACPH - Testimonial FormGautam50% (2)
- Concepts of DiseaseДокумент55 страницConcepts of DiseaseKailash NagarОценок пока нет
- Decision Making: Managing Risk: Summary of An Isop Workshop, Berlin, 2004Документ22 страницыDecision Making: Managing Risk: Summary of An Isop Workshop, Berlin, 2004Dipendra Ghimire100% (1)
- U S. Medical Eligibility Criteria For Contraceptive Use, 2010Документ77 страницU S. Medical Eligibility Criteria For Contraceptive Use, 2010gerte_yuewОценок пока нет
- Medical AffixДокумент6 страницMedical AffixOlib OlieОценок пока нет
- Wednesday SomersДокумент57 страницWednesday SomersNational Press FoundationОценок пока нет
- Resume Viola RDHДокумент2 страницыResume Viola RDHapi-247540600Оценок пока нет
- MSDSДокумент4 страницыMSDSkomite k3rsОценок пока нет
- 12 Questions To Help You Make Sense of A Diagnostic Test StudyДокумент6 страниц12 Questions To Help You Make Sense of A Diagnostic Test StudymailcdgnОценок пока нет
- National Mastitis Council 2018Документ137 страницNational Mastitis Council 2018Lysett CoronaОценок пока нет