Вам также может понравиться
- CoverДокумент16 страницCoverdiarОценок пока нет
- 2174-Article Text-18533-3-10-20191231 PDFДокумент10 страниц2174-Article Text-18533-3-10-20191231 PDFveliadwianditaОценок пока нет
- Peran Ayah Pada Praktek Pemberian Asi EksklusifДокумент10 страницPeran Ayah Pada Praktek Pemberian Asi EksklusifSatriaBajaОценок пока нет
- Kompres Jahe Merah Berpengaruh Terhadap Penurunan Skala Nyeri Osteoartritis Pada Lanjut Usia Di Wilayah Kerja Puskesmas Kampung Delima TAHUN 2016Документ9 страницKompres Jahe Merah Berpengaruh Terhadap Penurunan Skala Nyeri Osteoartritis Pada Lanjut Usia Di Wilayah Kerja Puskesmas Kampung Delima TAHUN 2016diarОценок пока нет
- Kompres Jahe Merah Berpengaruh Terhadap Penurunan Skala Nyeri Osteoartritis Pada Lanjut Usia Di Wilayah Kerja Puskesmas Kampung Delima TAHUN 2016Документ9 страницKompres Jahe Merah Berpengaruh Terhadap Penurunan Skala Nyeri Osteoartritis Pada Lanjut Usia Di Wilayah Kerja Puskesmas Kampung Delima TAHUN 2016diarОценок пока нет
- Health Promotion Related To HIVДокумент1 страницаHealth Promotion Related To HIVdiarОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- 2nd PartДокумент35 страниц2nd PartshahdatzОценок пока нет
- Yaya: Philippine Domestic Care Workers, The Children They CareДокумент18 страницYaya: Philippine Domestic Care Workers, The Children They CareAaliyahОценок пока нет
- Ashas New Pbi Format From June 2020Документ6 страницAshas New Pbi Format From June 2020phc kallumarriОценок пока нет
- Owner Torres": Registered The The PurposeДокумент1 страницаOwner Torres": Registered The The PurposeEl FiliОценок пока нет
- Breast FeedingДокумент12 страницBreast FeedingRiTa KathayatОценок пока нет
- A Petition For Divorce by Mutual Consent Us 13 (B) of The Hindu Marriage Act, 1955-1106Документ2 страницыA Petition For Divorce by Mutual Consent Us 13 (B) of The Hindu Marriage Act, 1955-1106naresh100% (1)
- 02 Gritzner JapanДокумент15 страниц02 Gritzner JapanVivian WangОценок пока нет
- CHN LEC 1 Week 5-6Документ39 страницCHN LEC 1 Week 5-6Carl Josef C. GarciaОценок пока нет
- Filipino ValuesДокумент16 страницFilipino ValuesKiel100% (1)
- The Pastoral Office, Divorce and RemarriageДокумент8 страницThe Pastoral Office, Divorce and RemarriageBror EricksonОценок пока нет
- Module 3 - SociologyДокумент74 страницыModule 3 - SociologyakshayaОценок пока нет
- Ancestral Veneration in The Yorùbá TraditionДокумент7 страницAncestral Veneration in The Yorùbá TraditionDarasia Selby91% (22)
- Hola AmigosДокумент1 страницаHola AmigosOscar Andres Alvarez MarinОценок пока нет
- Maternal Child Nursing Care in Canada 2nd Edition Perry Test BankДокумент8 страницMaternal Child Nursing Care in Canada 2nd Edition Perry Test Bankkevincharlesfztodrpwck100% (17)
- Great Answers To Difficult Questions About Adoption What Children Need To Know Great Answers To Difficult QueДокумент114 страницGreat Answers To Difficult Questions About Adoption What Children Need To Know Great Answers To Difficult QueVASCHOTI TRABANICOОценок пока нет
- East Sussex Domestic Violence and Abuse Protocol For Schools May 2016Документ26 страницEast Sussex Domestic Violence and Abuse Protocol For Schools May 2016liberto21Оценок пока нет
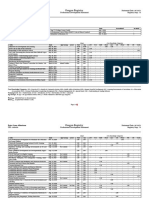
- Oregon Registry: Verified SubmissionsДокумент7 страницOregon Registry: Verified Submissionsapi-560491685Оценок пока нет
- School Form 2 (SF 2)Документ3 страницыSchool Form 2 (SF 2)Lorgin nunialaОценок пока нет
- The Influence of Parents Peers On The Moral Education of The Students at Notre Dame of Midsayap CollegeДокумент32 страницыThe Influence of Parents Peers On The Moral Education of The Students at Notre Dame of Midsayap CollegeStephen Jhone L. LibosadaОценок пока нет
- Family Life CycleДокумент8 страницFamily Life Cycleyaji ezraОценок пока нет
- MNДокумент2 страницыMNShahbaz Malbari100% (2)
- Enacting The AntiДокумент9 страницEnacting The AntimaryryomaОценок пока нет
- BERLIANA PUTRI - English For NurshingДокумент2 страницыBERLIANA PUTRI - English For NurshingPUTRI AYU PRIHATINIОценок пока нет
- NIBEDITA SAHU-final ThesisДокумент78 страницNIBEDITA SAHU-final ThesisSuman AgrawalОценок пока нет
- St. Lawrence County DSS Report From OCFSДокумент33 страницыSt. Lawrence County DSS Report From OCFSNorth Country This Week100% (1)
- Minutes of The Meeting of The Members of The Gad Focal Point System (GFPS) Held On February 7, 2022 at The Barangay Hall, Centro, Mandaue City.Документ2 страницыMinutes of The Meeting of The Members of The Gad Focal Point System (GFPS) Held On February 7, 2022 at The Barangay Hall, Centro, Mandaue City.Barangay Centro100% (4)
- Kinship 06Документ24 страницыKinship 06Saif RayhanОценок пока нет
- TEMPLATE PUBLIC SPEAKING OUTLINE FINAL EXAM 23 00 Walter UgazonДокумент3 страницыTEMPLATE PUBLIC SPEAKING OUTLINE FINAL EXAM 23 00 Walter Ugazonw1125jОценок пока нет
- MCP NCP Benefits SlidesДокумент13 страницMCP NCP Benefits SlidesJonas Marvin AnaqueОценок пока нет
- Sociological Analysis of Divorce: A Case Study From Pokhara, NepalДокумент9 страницSociological Analysis of Divorce: A Case Study From Pokhara, NepalNifaz KhanОценок пока нет