Вам также может понравиться
- Tranexamic Acid Injection 500 MG/ 5 ML Ampoule New Zealand Data SheetДокумент19 страницTranexamic Acid Injection 500 MG/ 5 ML Ampoule New Zealand Data Sheetkashif akhtarОценок пока нет
- TranexamicacidinjДокумент29 страницTranexamicacidinjPensayo, Stephanie Keith V.Оценок пока нет
- EC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1Документ11 страницEC-DH Epirubicin Cyclophosphamide Followed by Docetaxel With Trastuzumab Protocol V1.1smokkerОценок пока нет
- Hemostan LineInsert - Asean 2010Документ2 страницыHemostan LineInsert - Asean 2010Maybs Palec Pamplona-ParreñoОценок пока нет
- NICU Drugs GuideДокумент49 страницNICU Drugs GuideArhanОценок пока нет
- Docetaxel Carboplatin Trastuzumab T Carbo H Breast Cancer Adjuvant ProtocolДокумент14 страницDocetaxel Carboplatin Trastuzumab T Carbo H Breast Cancer Adjuvant ProtocolsmokkerОценок пока нет
- Paclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0Документ7 страницPaclitaxel With Dose Dense EC Adjuvant or Neo-Adjuvant Protocol V1.0smokkerОценок пока нет
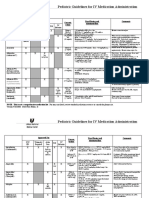
- Pediatric Guidelines For Medications PDFДокумент24 страницыPediatric Guidelines For Medications PDFLaylatan NurОценок пока нет
- New drugs in anesthesia - Sugammadex, Cis-atracurium, Remifentanyl, PalonosetronДокумент28 страницNew drugs in anesthesia - Sugammadex, Cis-atracurium, Remifentanyl, PalonosetronSai TejeswiОценок пока нет
- Data Sheet Hospira™ Tranexamic Acid Injection: PresentationДокумент17 страницData Sheet Hospira™ Tranexamic Acid Injection: PresentationAkhmad Rafi'iОценок пока нет
- Salbutamol Inhaler and Nebulizer InformationДокумент36 страницSalbutamol Inhaler and Nebulizer InformationlolabayОценок пока нет
- Vancomycin Dosing and Monitoring in AdultsДокумент1 страницаVancomycin Dosing and Monitoring in AdultsjulialeoОценок пока нет
- Am Iog Lyco SidesДокумент2 страницыAm Iog Lyco Sidesthemega1111Оценок пока нет
- Con 1420782810247Документ7 страницCon 1420782810247AsetonitrileОценок пока нет
- New Zealand Data Sheet for Amoxiclav Multichem Powder InjectionДокумент17 страницNew Zealand Data Sheet for Amoxiclav Multichem Powder InjectiondoodrillОценок пока нет
- Pediatric Guidelines For MedicationsДокумент24 страницыPediatric Guidelines For MedicationsjonatasmartinezОценок пока нет
- Recommended Doses of Medications To Treat Children With An Acute Asthma ExacerbaДокумент3 страницыRecommended Doses of Medications To Treat Children With An Acute Asthma Exacerbaمعاذ الشريفОценок пока нет
- Tranexamic Acid Injection Product MonographДокумент16 страницTranexamic Acid Injection Product MonographAhmad Zuhyardi LubisОценок пока нет
- Annex I Summary of Product CharacteristicsДокумент28 страницAnnex I Summary of Product CharacteristicsEmma SinОценок пока нет
- SMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)Документ7 страницSMILE (Etoposide, Ifosfamide, Methotrexate and Dexamethasone)SolikinОценок пока нет
- Guideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesДокумент8 страницGuideline: Antibiotic Drug Monitoring: Aminoglycosides and GlycopeptidesKenRodulfReyesVillaruelОценок пока нет
- Adult Electrolyte Replacement Protocol - MCLN 0006 J PDFДокумент1 страницаAdult Electrolyte Replacement Protocol - MCLN 0006 J PDFCraigОценок пока нет
- Paclitaxel With EC Adjuvant or Neoadjuvant Protocol V1.1Документ7 страницPaclitaxel With EC Adjuvant or Neoadjuvant Protocol V1.1smokkerОценок пока нет
- Enoxaparin Sodium Injection I.PДокумент15 страницEnoxaparin Sodium Injection I.PSuhailansariОценок пока нет
- Vancomicin Guidelines PICUДокумент2 страницыVancomicin Guidelines PICUAnonymous 6iwMFwОценок пока нет
- Sugammadex - PIДокумент15 страницSugammadex - PIveliaberlianaОценок пока нет
- Tranexamic Acid Injection AntifibrinolyticДокумент2 страницыTranexamic Acid Injection AntifibrinolyticUtari DesyaОценок пока нет
- Heparin Dose Adjustment in The Prescence of Renal ImpairmentДокумент5 страницHeparin Dose Adjustment in The Prescence of Renal ImpairmentRPR KSVОценок пока нет
- Core Safety ProfileДокумент13 страницCore Safety ProfileneleatucicovshiiОценок пока нет
- Aida Protocol For Apl: InductionДокумент4 страницыAida Protocol For Apl: InductionGabrielОценок пока нет
- Medication Administration PolicyДокумент188 страницMedication Administration Policyليراث ليОценок пока нет
- Atracurium MedscapeДокумент2 страницыAtracurium MedscapeKania DeazaraОценок пока нет
- Paclitaxel Trastuzumab Breast Cancer ProtocolДокумент9 страницPaclitaxel Trastuzumab Breast Cancer ProtocolsmokkerОценок пока нет
- Navelbine capsules guide for lung and breast cancerДокумент2 страницыNavelbine capsules guide for lung and breast cancerddandan_2Оценок пока нет
- DripsДокумент52 страницыDripsjanoloОценок пока нет
- Atropine: IndicationДокумент2 страницыAtropine: IndicationgugicevdzoceОценок пока нет
- K25. Malaria Pada AnakДокумент39 страницK25. Malaria Pada AnakayapillaiОценок пока нет
- Trastuzumab (Intravenous) Including Biosimilars of Trastuzumab - Drug Information - UpToDateДокумент20 страницTrastuzumab (Intravenous) Including Biosimilars of Trastuzumab - Drug Information - UpToDateDenys Romero100% (1)
- Merck Manual: Professional VersionДокумент25 страницMerck Manual: Professional VersionDwina Wiranti PutriОценок пока нет
- REGLAN Injection (Metoclopramide Injection, USP) RX OnlyДокумент15 страницREGLAN Injection (Metoclopramide Injection, USP) RX OnlydpkkrsterОценок пока нет
- RocuroniumbromideinjДокумент14 страницRocuroniumbromideinjagnes hutabaratОценок пока нет
- Actilyse ® 50 MG Actilyse ® 20 MG: Acute Myocardial InfarctionДокумент13 страницActilyse ® 50 MG Actilyse ® 20 MG: Acute Myocardial InfarctionmasterОценок пока нет
- Drug Doses & Frequency (Nicu) .12.mayДокумент20 страницDrug Doses & Frequency (Nicu) .12.mayTulasi100% (2)
- GDL 01240Документ7 страницGDL 01240Christian KosiОценок пока нет
- Perjeta Epar Product Information - enДокумент43 страницыPerjeta Epar Product Information - enGeo GeoОценок пока нет
- OB Hem Uterotonic Medications For Prevention and Treatment of PPHДокумент7 страницOB Hem Uterotonic Medications For Prevention and Treatment of PPHpwytymbm56Оценок пока нет
- Lsuhsc Nursing Licensed Personnel Inpatient RN Pharmacology Exam InstructionsДокумент10 страницLsuhsc Nursing Licensed Personnel Inpatient RN Pharmacology Exam Instructionskellly100% (1)
- Chemotherapy protocols for trophoblastic neoplasiaДокумент3 страницыChemotherapy protocols for trophoblastic neoplasiaImam Hakim SuryonoОценок пока нет
- Cisplatin-Pemetrexed (NSCLC)Документ5 страницCisplatin-Pemetrexed (NSCLC)Sindu SankarОценок пока нет
- Agatha Christie - Craciunul Lui PoirotДокумент14 страницAgatha Christie - Craciunul Lui PoirotIokan DanОценок пока нет
- Answers To Practice Problem Set #10Документ3 страницыAnswers To Practice Problem Set #10Raju NiraulaОценок пока нет
- Cilastati Imipenem Drug InfoДокумент19 страницCilastati Imipenem Drug InfoCosmina GeorgianaОценок пока нет
- Neoadjuvant or Adjuvant Therapy for Breast Cancer Using DOCEtaxel, CARBOplatin, and TrastuzumabДокумент6 страницNeoadjuvant or Adjuvant Therapy for Breast Cancer Using DOCEtaxel, CARBOplatin, and TrastuzumabMohammed GazoОценок пока нет
- First Selective Relaxant Binding Agent Sugammadex: Clinical PharmacologyДокумент9 страницFirst Selective Relaxant Binding Agent Sugammadex: Clinical PharmacologyyoshiudaОценок пока нет
- Aminoglycoside & VancomycinДокумент10 страницAminoglycoside & VancomycinKhor Chin PooОценок пока нет
- Endometrialcarcinoma r0416 7941Документ2 страницыEndometrialcarcinoma r0416 7941crisibarra911Оценок пока нет
- Azithromycin Monograph - PaediatricДокумент7 страницAzithromycin Monograph - PaediatrictynОценок пока нет
- Magnesium SulfateДокумент5 страницMagnesium SulfateRyan Inapan100% (1)
- Pharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamОт EverandPharmacy Calculation Workbook: 250 Questions to Prepare for the NAPLEX and PTCB ExamРейтинг: 5 из 5 звезд5/5 (1)
- To DownloadДокумент1 страницаTo DownloadHatim DziauddinОценок пока нет
- ATLS Practice Test 1: Other ThanДокумент11 страницATLS Practice Test 1: Other ThanGarcia Rosa75% (8)
- ATLS MCQs PDFДокумент4 страницыATLS MCQs PDFMohammad Abdulla70% (10)
- TicketsДокумент1 страницаTicketsHatim DziauddinОценок пока нет
- Airport Display SolutionsДокумент16 страницAirport Display SolutionsHatim DziauddinОценок пока нет
- National Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFДокумент247 страницNational Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFfghjОценок пока нет
- OctreotideДокумент3 страницыOctreotideHatim DziauddinОценок пока нет
- National Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFДокумент247 страницNational Antibiotic Guideline 2014 Full Versionjun2015 - 1 PDFfghjОценок пока нет
- TicketsДокумент1 страницаTicketsHatim DziauddinОценок пока нет
- Ucm 467056Документ47 страницUcm 467056Harmit Singh Bindra100% (1)
- Rapid Sequence Intubation: Mask and MonitoringДокумент6 страницRapid Sequence Intubation: Mask and MonitoringHatim DziauddinОценок пока нет
- 2014 Month CalendarДокумент12 страниц2014 Month CalendarAshari FathahillahОценок пока нет
- Bromhexine Tablet Syrup Elixir PDFДокумент4 страницыBromhexine Tablet Syrup Elixir PDFArthana PutraОценок пока нет
- Unstable Angina and NSTEMI: Early Unstable Angina and NSTEMI: Early Management ManagementДокумент30 страницUnstable Angina and NSTEMI: Early Unstable Angina and NSTEMI: Early Management ManagementHatim DziauddinОценок пока нет
- Tranexamic Acid Injection 500 MG/ 5 ML Ampoule New Zealand Data SheetДокумент18 страницTranexamic Acid Injection 500 MG/ 5 ML Ampoule New Zealand Data SheetHatim DziauddinОценок пока нет
- Office 2013 SP1 x64 Nov2014Документ1 страницаOffice 2013 SP1 x64 Nov2014Hatim DziauddinОценок пока нет
- DCOM 2015 Registration FormДокумент2 страницыDCOM 2015 Registration FormHatim DziauddinОценок пока нет
- Exam Dates Final Candidates 2015Документ2 страницыExam Dates Final Candidates 2015Hatim DziauddinОценок пока нет
- Critical Therapy Study ResultsДокумент4 страницыCritical Therapy Study ResultsAinur 'iin' RahmahОценок пока нет
- Hecat Module SHДокумент70 страницHecat Module SHHatim DziauddinОценок пока нет
- GINA Report 2015 Aug11Документ149 страницGINA Report 2015 Aug11Alex Medina AguilarОценок пока нет
- Teaching Feb 2015Документ3 страницыTeaching Feb 2015Hatim DziauddinОценок пока нет
- CPG Management of Hypertension (3rd Edition)Документ44 страницыCPG Management of Hypertension (3rd Edition)patricktiew100% (2)
- What Is A Dental AbscessДокумент10 страницWhat Is A Dental AbscessHatim Dziauddin100% (1)
- Health Issues Facing Adolescents in IndiaДокумент51 страницаHealth Issues Facing Adolescents in IndiaJerome Manaig SueltoОценок пока нет
- Urology: Magazine For Companion-Animal PractitionersДокумент48 страницUrology: Magazine For Companion-Animal PractitionersJuan Carlos Ortiz RamirezОценок пока нет
- Anal FissuresДокумент2 страницыAnal FissureskhadzxОценок пока нет
- Best Pulmonologist in Velachery - Sabari Lung Care Clinic - Reasearch PaperДокумент2 страницыBest Pulmonologist in Velachery - Sabari Lung Care Clinic - Reasearch PaperSabari Lung Care ClinicОценок пока нет
- Maharashtra University of Health Science, Nashik: Physiotherapy Syllabus III - B.P.THДокумент28 страницMaharashtra University of Health Science, Nashik: Physiotherapy Syllabus III - B.P.THDevasyaОценок пока нет
- G6PD COVID ReviewДокумент6 страницG6PD COVID Reviewnoordin othmanОценок пока нет
- Polidocanol Asclera Varithena National Drug Monograph FinalДокумент27 страницPolidocanol Asclera Varithena National Drug Monograph FinalbvarianoОценок пока нет
- Comprehensive Dental Management of Children With Henoch-Schonlein Purpura-Vera YulinaДокумент22 страницыComprehensive Dental Management of Children With Henoch-Schonlein Purpura-Vera YulinaShinta Dewi NОценок пока нет
- ABC of arterial and venous disease: Chronic lower limb ischaemiaДокумент4 страницыABC of arterial and venous disease: Chronic lower limb ischaemiaTaufik Gumilar WahyudinОценок пока нет
- Causes and Types of AscitesДокумент40 страницCauses and Types of AscitesJavaid KhanОценок пока нет
- Vol 1 50 TEST IIДокумент11 страницVol 1 50 TEST IIMaria Zm LatonОценок пока нет
- VertigoДокумент84 страницыVertigoartika mayandaОценок пока нет
- QuestionsДокумент21 страницаQuestionsashaaman0325Оценок пока нет
- Neuro ReviewerДокумент41 страницаNeuro ReviewerKyla Shain GallegoОценок пока нет
- 急性呼吸障害を来した単純ヘルペス脳炎 において脳幹病変が病理学的に確認でき た 89 歳男性の 1 例 A case of an 89-year-old male with pathologically confirmed brainstem lesion in herpes simplex encephalitis with acute respiratory disorderДокумент6 страниц急性呼吸障害を来した単純ヘルペス脳炎 において脳幹病変が病理学的に確認でき た 89 歳男性の 1 例 A case of an 89-year-old male with pathologically confirmed brainstem lesion in herpes simplex encephalitis with acute respiratory disorderEdgar Azael GarciaОценок пока нет
- Sal But AmolДокумент2 страницыSal But AmolCalimlim KimОценок пока нет
- Extrapyramidal Disorders, OedemaДокумент104 страницыExtrapyramidal Disorders, OedemaAyman RehmanОценок пока нет
- Hematology: For Students and PractitionersДокумент699 страницHematology: For Students and PractitionersRebeenMustafa100% (1)
- 4 - LDC Revised Grading of Acute Kidney Injury (1 5)Документ7 страниц4 - LDC Revised Grading of Acute Kidney Injury (1 5)kradoОценок пока нет
- Lung ExaminationДокумент14 страницLung Examinationსალომე მუმლაძე “Slay” TMAОценок пока нет
- Clinical Liver Disease - 2021 - Sharma - Liver Abscess Complications and TreatmentДокумент5 страницClinical Liver Disease - 2021 - Sharma - Liver Abscess Complications and TreatmentMuhammad RifkiОценок пока нет
- SINGAPORE CPG - Blood Transfusion FinalДокумент97 страницSINGAPORE CPG - Blood Transfusion FinalSamuel Ravi ChoudhuryОценок пока нет
- Incidence of Glaucoma in Patients Using Topical Steroids Eye DropsДокумент3 страницыIncidence of Glaucoma in Patients Using Topical Steroids Eye DropsAnonymous kDoZoLОценок пока нет
- DSM V Clinical Cases - Chapter 12 Sleep Wake DisordersДокумент13 страницDSM V Clinical Cases - Chapter 12 Sleep Wake DisordersIzzyinOzzieОценок пока нет
- Nursing Care Plan: Course InstructorsДокумент11 страницNursing Care Plan: Course InstructorsFatema AlsayariОценок пока нет
- CCHM 311 Week 1617 Liver FunctionДокумент10 страницCCHM 311 Week 1617 Liver FunctionMax RuideraОценок пока нет
- Reviews: Epidemiology, Definition and Treatment of Complicated Urinary Tract InfectionsДокумент15 страницReviews: Epidemiology, Definition and Treatment of Complicated Urinary Tract InfectionsPutu AdiОценок пока нет
- Liver DiseasesДокумент114 страницLiver DiseasesDayang Feineliza Samman BahjinОценок пока нет
- Cervico-Cranial Red Flag Tool - Final For SoMeДокумент1 страницаCervico-Cranial Red Flag Tool - Final For SoMeDavid StreisselОценок пока нет
- Multiple SclerosisДокумент13 страницMultiple SclerosisGEETA MOHANОценок пока нет