Академический Документы
Профессиональный Документы
Культура Документы
54 103 1 SM
Загружено:
EviОригинальное название
Авторское право
Доступные форматы
Поделиться этим документом
Поделиться или встроить документ
Этот документ был вам полезен?
Это неприемлемый материал?
Пожаловаться на этот документАвторское право:
Доступные форматы
54 103 1 SM
Загружено:
EviАвторское право:
Доступные форматы
CLINICAL NURSES FORUM
NONPHARMACOLOGIC PEDIATRIC PAIN
MANAGEMENT IN EMERGENCY DEPARTMENTS:
A SYSTEMATIC REVIEW OF THE LITERATURE
Author: Sarah J. K. Wente, PhD, RN, Richfield, MN
Section Editor: Andrew D. Harding, MS, RN, CEN, NEA-BC, FAHA, FACHE
Earn Up to 9.0 CE Hours. See page 212.
Introduction: Children account for numerous ED visits each explored cold application, and 1 looked at parental holding and
year, with the majority of children reporting pain or requiring positioning. Benefits of using nonpharmacological methods
painful procedures. The fast-paced, noisy environment, varying included decreased pain, distress, and anxiety reported by the
resources, and staff trained in taking care of pediatric patients parent, child, and/or observer.
make the ED a unique place to care for children in pain.
Discussion: Findings suggest nonpharmacological inter-
Nonpharmacological interventions are an essential part of pain
ventions such as distraction, positioning, sucrose, and cold
management. The purpose of this review was to examine what
application may be helpful in pediatric pain management
nonpharmacological interventions EDs are using for pain
in the ED. Nurses can implement these methods indepen-
management in children ages birth to 18 years.
dently when caring for children and their families. In
Methods: A systematic literature search was conducted to addition, nonpharmacological methods are relatively inex-
examine nonpharmacological interventions used for pain pensive to organizations.
management of children in EDs.
Results: Fourteen articles met the inclusion/exclusion criteria. Key words: Emergency department; Pediatric; Nonpharmaco-
Ten studies used distraction, 2 examined the use of sucrose, 1 logical pain management; Systematic literature review
pproximately one-third of patients visiting the mentation of nonpharmacologic and pharmacologic inter-
A emergency department are children and adolescents.
Seventy-seven percent of patients presenting to the
emergency department are in pain and/or require painful
vention best practices, often leads to optimal pain
management for children. Although a significant amount
of pharmacologic best practice exists, evidence regarding
procedures. 1-3 Busy, noisy emergency departments and nonpharmacologic interventions is not well-known and not
limited pediatric resources and/or staff trained in caring for always incorporated into the delivery of everyday patient
these patients, combined with acuity, create a set of unique care. Therefore the purpose of this article is to present a
challenges for the patient, family, and care providers. 4-6 A systematic literature review regarding nonpharmacologic
prompt and thorough assessment, combined with imple- pain management techniques provided for children, from
birth to age 18 years, seeking ED care.
Overview of Nonpharmacologic Pain Management
Sarah J. K. Wente is Adjunct Faculty, College of Nursing, Globe University/
Minnesota School of Business, Richfield, MN. Nonpharmacologic pain management is a broad term and
For correspondence, write: Sarah J. K. Wente, PhD, RN, College of Nursing, encompasses those interventions that do not use pharma-
Globe University/Minnesota School of Business, 1401 West 76th Street, cologic methods to treat pain. These types of interven-
Richfield, MN 55423; E-mail: swente@msbcollege.edu. tions are an “integral part of the care of all children
J Emerg Nurs 2013;39:140-50. experiencing pain” 7 and include cognitive-behavioral and
Available online 28 November 2012.
physical approaches. Cognitive-behavioral approaches actively
0099-1767/$36.00
Copyright © 2013 Emergency Nurses Association. Published by Elsevier Inc. engage children and help them to redirect their attention away
All rights reserved. from fearful and painful procedures. 8 Examples of cognitive-
http://dx.doi.org/10.1016/j.jen.2012.09.011 behavioral interventions include music, guided imagery,
140 JOURNAL OF EMERGENCY NURSING VOLUME 39 • ISSUE 2 March 2013
Wente/CLINICAL NURSES FORUM
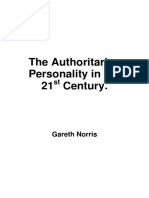
Records identified from Additional records through article
database search reference lists
CINAHL 221 4
PubMed 1133
Total 1354
Number of records excluded
Number of records screened 1344
1358
Reasons for exclusion
• Study not conducted in ED
• Sample >18 years
• Pharmacological
Number of studies included in the
intervention
systematic review 14
• Expert Opinion
FIGURE
Search results.
distraction, hypnosis, relaxation techniques, controlled Systematic Literature Search
breathing, and biofeedback exercises. 8 Nonpharmacologic
physical approaches include hot and cold application, The purpose of this systematic literature review was to
massage, stroking, swaddling, sucking, splinting, acupunc- address the following question: What nonpharmacologic
ture, temperature regulation, and transcutaneous electrical interventions are emergency departments using for pain
nerve stimulation, 1,9,10 as well as cutaneous stimulation to management in children? CINAHL (Cumulative Index to
reduce pain perception. 11 Nursing and Allied Health Literature), PubMed, and the
The goals of nonpharmacologic interventions are to Cochrane database were searched. To capture pain manage-
decrease fear, reduce distress and pain, and give children a ment practices after the release of the Agency for Healthcare
sense of control. 8 Both physical and cognitive-behavioral Policy and Research (now known as the Agency for
approaches are essential to providing a comfortable environ- Healthcare Research and Quality) guideline, 20 articles
ment for the child. 12 In addition, using nonpharmacologic were limited to those published between January 1, 1995,
interventions during medical procedures has been found to and December 1, 2010. All research articles involving
reduce the stress experienced by parents, and nurses can nonpharmacologic interventions with children aged 0 to 18
independently implement these practices and encourage years in emergency departments were included. Articles were
family members to actively participate in the patients’ care. excluded if they were not published in English, focused
Incorporating nonpharmacologic interventions should be an solely on pharmacologic interventions, included adults only,
essential part of pediatric pain management in the emergency and/or addressed prehospital or inpatient pain strategies. A
department, alone or in conjunction with pharmacologic search of PubMed, CINAHL, and the Cochrane database
measures based on the needs of the child. yielded a total of 1,354 articles, and 10 articles met the
The choice of nonpharmacologic interventions varies inclusion/exclusion criteria. Reference lists of the 10
by the age of the child and developmental factors. Common identified articles were also reviewed, and 4 additional
nonpharmacologic interventions for infants in pain include articles met the inclusion/exclusion criteria. Thus a total
pacifiers, swaddling, holding, rocking, singing/music, and of 14 articles were identified that met the inclusion/
sucrose via pacifier, syringe, or gloved finger. 9,10,13-19 exclusion criteria for this review. The Figure displays
Distraction using toys and books is often used for younger the search process. Seven of these studies used an
children, whereas older children may use video games or experimental randomized controlled design, five used a
computers. Physical strategies that are beneficial to children quasi-experimental design, and two were descriptive studies.
and adolescents include hot or cold application, pressure, The majority of studies (n = 10) compared responses in a
massage, acupuncture, or immobilization. 1,9 group of children who received a nonpharmacologic
March 2013 VOLUME 39 • ISSUE 2 WWW.JENONLINE.ORG 141
CLINICAL NURSES FORUM/Wente
142
TABLE
JOURNAL OF EMERGENCY NURSING
Summary of articles included in systematic literature search
Author Type of Type of Type of study Sample Outcome Instruments Results
intervention procedure variables
Carlson et al 27 Distraction Venipuncture 2-Group 384 Pain, distress, VAS-fear scale, No difference was found
(2000) using illusion or IV line randomized children, and fear PRS-R, between the control and
kaleidoscope insertion design aged 4-18 y, Oucher scale kaleidoscope groups for
13 sites observed behavioral distress
or child self-report of pain
and fear. No significant
differences were found
between the kaleidoscope
and control groups in
parent or nurse ratings
of fear.
Cavender Distraction using Venipuncture Experimental 43 children, Pain, fear, FACES, The experimental group
et al 28 choice of or IV line comparison aged 4-11 y and distress Glasses showed significantly lower
(2004) kaleidoscope, insertion group Fear Scale, fear compared with the
I Spy book, or PBCL control group as reported
Thomas the by CLS and parents
Tank lift and (P = .003, P b .001). No
flap book and significant difference was
parental found between child's
positioning self-report of pain or fear.
(side sitting or No difference in behavioral
chest to chest) distress was found between
groups as rated by the CLS.
Curtis et al 37 Sucrose, placebo, Venipuncture RCT 84 infants, Pain, crying FLACC On the basis of unadjusted
(2008) pacifier and sucrose, aged 0-6 mo time, and scale effects analysis, the pacifier
pacifier and placebo heart rate group showed decreased
change from pain compared with the
baseline group using no pacifier;
VOLUME 39 • ISSUE 2
the difference was not
significant (P = .06). On
unadjusted analysis, the
sucrose group was not
found to significantly affect
FLACC score change,
crying time, or heart rate.
March 2013
Regression analysis adjusted
for age showed that sucrose
compared with placebo
(P = .01) and pacifier
March 2013
compared with no pacifier
(P b .0001) yielded
significantly shorter
crying times.
Goymour Play therapist Venipuncture Control/ 100 children, Parent/child Author- The play therapy group was
VOLUME 39 • ISSUE 2
et al 29 using or cannulation intervention, aged 4-15 y rating of child designed significantly more prepared
(2000) distraction vs randomization preparedness, questionnaire (P b .001) and had a
standard care unknown child's distress, for parent significantly lower rating
and staff ease and child to of distress before, during,
jointly rate, and after the procedure
as well as compared with the standard
medical staff care group (P = .001,
member P b .001, and P = .002,
respectively). Medical
staff perceived the procedure
as quicker and easier when
the play therapist was present.
Malone 30 Distraction with IV line insertion, Equivalent 40 children, Behavioral Predominant Music intervention groups
(1996) music venipuncture, and matched aged 0-7 y distress Behavior showed significantly less
intervention injections, on age, Categories behavioral distress during
heel sticks procedure, List pre-needle and post-needle
and type of stages compared with
insertion the control group
(P b .05). In the music
group, children aged 0
to 1 y showed significantly
less distress during music
than older age groups
(P b .05).
Movahedi Cold therapy Venipuncture Quasi- 80 children, Physiological, CHEOPS, There were no significant
et al 11 experimental, aged 6-12 y behavioral, Oucher differences in physiological
(2006) treatment/ and scale, blood responses between groups
control subjective pressure, before or after procedure.
responses heart rate, The treatment group with
Wente/CLINICAL NURSES FORUM
WWW.JENONLINE.ORG
and an ice bag applied had
respiratory significantly less pain
rate behavioral responses
(P = .001) and self-reported
pain after the procedure
(P = .0097) than the
control group.
(continued on next page)
143
CLINICAL NURSES FORUM/Wente
144
TABLE
Continued
JOURNAL OF EMERGENCY NURSING
Author Type of Type of Type of study Sample Outcome Instruments Results
intervention procedure variables
Press et al 31 Active distraction Venipuncture Randomized 94 children, Pain and VAS combined There was no significant
(2003) via music controlled aged 6-16 y procedure with pain difference between
combined design duration face scale experimental and control
with uncertainty groups after controlling for
reduction confounding variables
of age and pain threshold.
No difference in duration
of procedure was found
between groups. Interactions
identified that in the
experimental group, female
patients reported lower pain
levels than girls in the control
group (P b .01); children
in the experimental group
reported lower pain levels
than controls only in children
with higher sensitivity
to pain (P b .05); and
children with a white blood
cell count of b 12,000 in the
experimental group reported
significantly lower pain
than those in the control group
(P b .05).
Rogers et al 38 Sucrose Bladder RCT, randomized 80 infants, Pain, crying DAN scoring Overall, no significant difference
(2006) catheterization double blinded aged b 90 d time, and system, a was found between the placebo
behavior measure of and control groups in pain
infant scores and crying time.
VOLUME 39 • ISSUE 2
behavioral Subgroup analysis showed
responses that infants aged 1 to 30 d
to pain had less pain (P = .035),
were significantly less likely
to cry during the procedure
(P = .008), and returned
to baseline behavior sooner
March 2013
(P = .04) after catheter removal
compared with the placebo
group. For infants aged N 30 d,
there was no difference
March 2013
between groups in pain scores,
crying time, or return to
baseline behavior.
Sinha et al 32 Distraction using Laceration repair Random 240 children, Pain, distress, FPS, VAS for No difference in pain was
(2006) age-appropriate assignment aged 6-18 y and anxiety distress, and found between the control
VOLUME 39 • ISSUE 2
items including to control STAIC and intervention groups
music, video or invention for all children. Children
games, cartoon group aged b 10 y had a significant
videos, books, difference in distress as
or blowing reported by the parent
bubbles (P = .01); distress was lower
in the intervention group.
Anxiety was significantly
less in the intervention group
for children aged ≥10 y
(P b .001). There was no
difference in distress as
reported by the parent for
children aged ≥10 y.
Sobieraj et al 33 Distraction using Simple laceration Quasi- 57 children, Distress and PBCL and No difference was found in
(2009) music, parents repair experimental aged parental parental parental participation between
were encouraged 12-71 mo participation participation the control and intervention
to sing along during score (time groups. There were no
procedure distracting/ significant differences in
total procedure distress scores between the
time) intervention and control
groups based on parental
participation. The greatest
predictors of distress in the
child were age (young
children were more distressed)
and the presence of the
father (more distress) during
the procedure. A significantly
Wente/CLINICAL NURSES FORUM
WWW.JENONLINE.ORG
higher mean distress score
was found if the father
was present compared with
when only the mother
was present (43.68 vs 23.39,
P b .001).
(continued on next page)
145
CLINICAL NURSES FORUM/Wente
146
JOURNAL OF EMERGENCY NURSING
TABLE
Continued
Author Type of Type of Type of study Sample Outcome Instruments Results
intervention procedure variables
Sparks et al 41 Parent holding IV line Randomized 118 infants/ Distress and PBRS-R and Significantly lower distress
(2007) and upright insertion experimental or children, parent and selected scores were found in the
positioning control group aged nurse items from experimental group during
of child 9-47 mo satisfaction PPSC all time periods (before,
during, and after) compared
with control (P b .001 to
P = .044); parents in the
experimental group reported
significantly greater satisfaction
with the child's position
(P = .034). Nurses reported
significantly greater satisfaction
with the child's position in
the control group (P b .001).
Tanabe 3 groups: standard Musculoskeletal Interventional 76 children, Pain and FACES, The group receiving standard
et al 34 care (ice, trauma study with aged 5-17 y patient numeric care and distraction had a
(2002) elevation, and systematic satisfaction rating scale, significant reduction in pain
immobilization), assignment and 2 patient ratings at 30 and 60 minutes
standard care to 1 of satisfaction (P b .05) compared with the
and ibuprofen, 3 groups questions group receiving standard
or standard care and the group receiving
care and distraction standard care and ibuprofen.
All groups had a significant
improvement in pain distress
from 0 to 30 minutes and at
60 minutes.
VOLUME 39 • ISSUE 2
Winskill Distraction boxes Not reported Descriptive 13 staff Use and Interview All responses indicated
et al 35 with age-appropriate resource benefits containing that, when used, distraction
(2008) toys people of distraction 5 questions boxes reduced pain and
boxes anxiety experienced by
children in the emergency
department; 6 people
reported that the use of
March 2013
distraction boxes decreased
the need for administration
of medications in children
needing procedures.
Wente/CLINICAL NURSES FORUM
FLACC, Face, Legs, Activity, Cry, Consolability; IV, intravenous; PBCL, Procedural Behavior Checklist; PBRS-R, Procedural Behavior Rating Scale, revised version; RCT, randomized controlled trial; PRS-R, Procedure Rating Scale-Revised; CHEOPS,
intervention with a control group who received standard care.
was found. Improved customer
service was shown by increased
additional benefit of decreased
distress and anxiety in parents Sample sizes ranged from 40 to 384 children. Studies were
music was “helpful” or “very
Children’s Hospital of Eastern Ontario Pain Scale; DAN, Douleur Aigue du Nouveau-ne´; FPS, Facial Pain Scale; STAIC, State Trait Anxiety Inventory for Children; PPSC, Parent Perceptions of Specialty Care; VAS, visual analog scale.
scores for pain management
pain and/or discomfort. An
conducted in the United States (n = 8), Canada, (n = 2),
and overall quality of care.
reported that listening to
Australia (n = 2), Israel (n = 1), and Iran (n = 1). A variety of
86% of patients/families
helpful” in decreasing
instruments were used to measure the outcomes of pain,
anxiety, fear, distress, and parental participation. Common
scales used to assess pain and distress were the FLACC (Face,
Legs, Activity, Cry, Consolability), 21 FACES, 22 Oucher
scale, 23,24 visual analog scale, 25 and Procedural Behavior
Rating Scale, revised version/Procedural Behavior Checklist. 26
Although little information exists specific to children in
emergency departments, the information on these scales
supports their use for assessment of pain in children in
Investigator-
4-question
emergency departments. The results of the systematic review
designed
survey
are presented, and the Table summarizes each article.
Nonpharmacologic Interventions Used
Patient/family
and families satisfaction
Distraction was the most common intervention used during
procedures to manage pain in children during their ED
visits. Ten studies described various distraction methods to
reduce pain, anxiety, and/or distress and increase parental
participation. 27-36 Five studies focused on 1 method of
distraction, such as music, 27,30,31,33,36 and five studies had
50 patients
more than 1 method of distraction available. 28,29,32,34,35 In
the 5 studies with only 1 method of distraction, the
distractor was selected by the researcher, whereas in the
other 5 studies, the child was allowed to choose. 28,29,32,34,35
Although research with a well-defined distraction interven-
Descriptive
tion allows an in-depth exploration of that particular
method, in practice, a variety of distractors for children to
select from takes into consideration their developmental
stages and preferences. However, exploring a combination
of interventions together makes it difficult to determine the
and painful
procedures
efficacy of the individual distractor.
Variety of
illnesses
Two studies examined the use of sucrose in infants in
the emergency department to reduce pain and distress. 37,38
Curtis et al 37 focused on sucrose during venipuncture,
whereas Rogers et al 38 looked at the effects of sucrose on
infants during bladder catheterization. In previous research,
sucrose has been primarily studied in the newborn nursery
with music
and neonatal intensive care unit. 39,40 Prior studies showed
Distraction
that infants given oral sucrose cried less and had a decreased
behavioral pain response compared with infants who
received a placebo during procedures. 39,40
Movahedi et al 11 were the only researchers to examine
the effect of local refrigeration, cold application, before
venipuncture on pain-related responses for school-aged
(2010)
et al 36
Young
children in the emergency department. Application of cold
is one method of cutaneous stimulation that has been used
to relieve pain and promote healing. In addition, applying
March 2013 VOLUME 39 • ISSUE 2 WWW.JENONLINE.ORG 147
CLINICAL NURSES FORUM/Wente
cold to an area is thought to slow the ability of pain fibers to were significantly less likely to cry during the procedure
transmit pain impulses. 21 (P = .008) and had a smaller change in pain scores (P = .035),
One study compared parental holding and upright indicating less pain, and their behavior returned to baseline
positioning of the child versus traditional supine positioning sooner after catheter removal (P = .04) compared with the
during intravenous insertion. 41 Alternative positioning for placebo group. Infants aged older than 30 days showed no
children during painful procedures has been recommended difference between groups in pain scores, crying time, or
as a method to comfort children. 42 return to baseline behavior. 33
Curtis et al 37 examined sucrose, placebo, and pacifier
Systematic Review Results use. They found that sucrose compared with placebo
(P = .01) and pacifier compared with no pacifier (P b .0001)
Study results of the use of distraction in emergency resulted in significantly less crying time when adjusting for
departments were mixed when using distraction as an age. The pacifier group showed a clinically significant change
intervention to reduce pain in children. Two descriptive in average FLACC (Face, Legs, Activity, Cry, Consolability)
studies described distraction as helpful for decreasing pain or score, and crying time was significantly reduced with pacifier
discomfort as reported by parents, children, or resource use versus no pacifier use in both younger groups (0-1
staff. 35,36 Approximately half of the resource staff interviewed month, P b .017; 1-3 months, P b .003).
reported that the use of distraction boxes—boxes in the The study by Movahedi et al 11 was the only one to
emergency department that contained selected age-appropri- examine the effect of “local refrigeration,” cold application,
ate toys with instructions—reduced the need for pain on venipuncture pain in children. Results showed that
medication in children undergoing procedures and thought applying an ice bag 3 minutes before the procedure yielded
the use of the distraction boxes minimized anxiety and pain in a significant difference in observed behavioral responses
children in the emergency department. 35 Improved customer (P = .0011) and self-reported pain (P = .0097) compared
service shown by increased scores for pain management and with the control group.
overall quality of care was also found. 36 Sparks et al 41 looked at positioning and parent holding
Significantly less behavioral distress, decreased pain, and their impact on distress and satisfaction with the
and more prepared children were reported in 4 studies using procedure. At each of the 3 time periods (before, during, and
distraction. 29-31,34 Parents’ and child life specialist's (CLS) after the procedure), the intervention group had a significant
report of fear was significantly lower in the experimental reduction in child distress compared with the control group
group in one study (P b .001, P = .003), although no (P b .001 to P = .044). No difference was found in overall
difference was found for children's report of fear in this parent satisfaction, although significantly greater nurse
study. 28 Distress as perceived by the parent/guardian was satisfaction was reported in the control group (P b .001),
significantly less in the intervention group for children which included the child lying down for the procedure.
younger than 10 years of age during laceration repair (P =
.01), whereas no difference in distress was found when the
children's report of distress was analyzed. 32 In children 10 Implications for Research and Practice
aged years or older, situational anxiety was significantly less
in the intervention group compared with the noninterven- Nonpharmacologic interventions are crucial in caring for
tion group (P b .001). 32 Several studies reported additional infants and children. Although results from the studies
unique findings. Press et al 31 found an interaction effect for varied, positive outcomes of using methods such as dis-
gender and condition, with girls receiving distraction during traction, positioning and parent holding, sucrose, pacifier,
venipuncture. Girls in the experimental group reported and cold application included reduced distress, pain,
significantly less pain than girls in the control group anxiety, and behavioral response reported by the child,
(P b .01). Sobieraj et al 33 found that significantly higher parent, and/or observer. No negative outcomes were
distress scores were reported if the father was present than if reported, and nonpharmacologic interventions can be
only the mother was present during laceration repair (P b .001). implemented independently with little cost. Additional
Two researchers examined sucrose use in infants in the research on nonpharmacologic pain management in
emergency department, one during venipuncture and children in the emergency department is needed to further
another during bladder catheterization, and initially found explore the benefits children may receive from the use of
no significant differences in pain between the intervention nonpharmacologic approaches.
and control groups. 37,38 In the subgroup analysis of Rogers Using sucrose and/or a pacifier can be implemented
et al 38 of infants aged 1 to 30 days, infants receiving sucrose independently to reduce pain in infants and is fairly
148 JOURNAL OF EMERGENCY NURSING VOLUME 39 • ISSUE 2 March 2013
Wente/CLINICAL NURSES FORUM
inexpensive. Infant age and procedure type should be taken effective, and there is no evidence indicating that this
into consideration when implementing this intervention. technique is related to negative outcomes. Emergency
More research on infants aged younger than 60 days using departments should have a variety of distractors available
sucrose to reduce pain/distress associated with painful pro- for children of all ages. Having readily available resources
cedures in the emergency department is needed. The con- and information for nurses to use will help encourage the
centration of sucrose is an area to expand on to determine use of these methods.
the most appropriate concentration for the infant based on
size and age.
Several of the studies used CLSs to provide the inter-
Conclusion
vention and standard of care. Although CLSs are an integral
part of pain management in children, they are not available in Nonpharmacologic interventions are a vital part of caring
all emergency departments and may not be present on all shifts. for children in emergency departments and should be
CLSs have specialized training, and the results may differ if incorporated into clinical practice in conjunction with
other health care providers deliver the intervention. Additional pharmacologic measures or alone based on the assessment
research is needed examining the impact when other of the child. The busy environment, varying levels of
health care providers, such as nurses, deliver the intervention. pediatric experience and resources, and heightened time of
When appropriate, parents should be encouraged to crisis for children in emergency departments create
hold children in an upright position during procedures and additional challenges for providing pain management.
nurses may consider applying ice before intravenous Continued efforts are needed to ensure that children cared
insertion to reduce pain and distress in children. Factors for in emergency departments are provided adequate pain
such as patient condition, age, parent comfort level, and management using nonpharmacologic and pharmacologic
relationship with the child are some aspects to take into interventions. Additional research is needed to identify
account when one is using these methods. Additional environmental and organizational barriers that impede the
research on positioning and cold application is needed, implementation of nonpharmacologic interventions be-
including larger samples sizes and expanded ages. cause these data will enable nurses to integrate these
An important aspect of the use of nonpharmacologic techniques into their care routines.
interventions is the appropriate assessment of pain and the
use of this assessment to evaluate the effectiveness of the
intervention on reducing pain as well as distress in children. REFERENCES
Additional research is needed to examine the effectives of 1. Bauman BH, McManus JJ. Pediatric pain management in the emergency
instruments for children in the emergency department. Some department. Emerg Med Clin North Am. 2005;23(2):393-414.
of the studies combined more than 1 intervention; additional 2. Drendel AL, Brousseau DC, Gorelick MH. Pain assessment for pediatric
studies are needed to determine the impact of each specific patients in the emergency department. Pediatrics. 2006;117(5):1511-8.
nonpharmacologic approach on procedural pain, distress, 3. MacLean SL, Bayley EW, Cole FL, Bernardo L, Lenaghan P, Manton
and anxiety in children in the emergency department. A. The LUNAR project: a description of the population of individuals
The review discovered mixed results when distraction who seek health care at emergency departments…learning and using
was used as an intervention to reduce pain and distress in new approaches in research. J Emerg Nurs. 1999;25(4):269-82.
children in the emergency department. One reason for 4. Gausche-Hill M, Schmitz C, Lewis RJ. Pediatric preparedness of US
finding no significant difference between groups may be the emergency departments: a 2003 survey. Pediatrics. 2007;120(6):1229-37.
way in which intervention and control groups were carried 5. Ramponi D. Reducing pain in pediatric procedures in the emergency
out. Careful implementation and examination of both department. J Emerg Nurs. 2009;35(4):379-82.
intervention and control groups are needed to limit 6. Tracy MA. Improving pediatric quality care in general care emergency
treatment contamination. Several studies with no difference departments. J Emerg Nurs. 2007;33(4):399-401.
noted that the control group may have included parents that 7. Wise B, McKenna C, Garvin G, Harmon B, eds. Nursing Care of the
used distraction naturally, without prompting, or the General Pediatric Surgical Patient. New York: Aspen; 2000:60.
quality of the distraction may not have been sufficient to 8. Khan K, Weisman S. Nonpharmacologic pain management strategies in the
show a difference. 27,32,33 Further research is needed using pediatric emergency department. J Clin Pediatr Emerg Med. 2007;8:240-7.
larger sample sizes and examination of the fidelity of the 9. Burns C, Dunn A, Brady M, Starr N, Blosser C, eds. Pediatric Primary
intervention provided. Care. 4th ed. St Louis, Missouri: Saunders Elsevier; 2008:462-3.
Distraction is an intervention that can be provided 10. Wilson D, Hockenberry M, eds. Wong's Clinical Manual of Pediatric
with little training, it has minimal risk, and it is cost Nursing. 8th ed. St Louis, Missouri: Mosby; 2012:191-2.
March 2013 VOLUME 39 • ISSUE 2 WWW.JENONLINE.ORG 149
CLINICAL NURSES FORUM/Wente
11. Movahedi AF, Rostami S, Salsali M, Keikhaee B, Moradi A. Effect of 28. Cavender K, Goff MD, Hollon EC, Guzzetta CE. Parents’ positioning
local refrigeration prior to venipuncture on pain related responses in and distracting children during venipuncture: effects on children's pain,
school age children. Aust J Adv Nurs. 2006;24(2):51-5. fear, and distress. J Holist Nurs. 2004;22(1):32-56.
12. Zempsky WT, Cravero JP. Clinical report: relief of pain and anxiety in 29. Goymour K, Stephenson C, Goodenough B, Boulton C. Evaluating the
pediatric patients in emergency medical systems. Pediatrics. 2004;114(5): role of play therapy in the paediatric emergency department. Aust Emerg
1348-56. Nurs J. 2000;3(2):10-2.
13. Uman LS, Chambers CT, McGrath PJ, Kisely SR. Psychological 30. Malone B. The effect of live music on the distress of pediatric patients
interventions for needle-related procedural pain and distress in children receiving intravenous starts, venipunctures, injections, and heel sticks.
and adolescents. Cochrane Database Syst Rev. 2006;(4):CD005179. J Music Ther. 1996;33:19-33.
14. Kleiber C, Harper DC. Brief report. Effects of distraction on children's 31. Press J, Gidron Y, Maimon M, Gonen A, Goldman V, Buskila D.
pain and distress during medical procedures: a meta-analysis. Nurs Res. Effects of active distraction on pain of children undergoing venipunc-
1999;48(1):44-9. ture: who benefits from it? Pain Clin. 2003;15(3):261-9.
15. Cohen L, Blount R, Cohen R, Ball C, McClellan C, Bernard R. 32. Sinha M, Christopher NC, Fenn R, Reeves L. Evaluation of
Children's expectations and memories of acute distress: short- and long- nonpharmacologic methods of pain and anxiety management for
term efficacy of pain management interventions. J Pediatr Psychol. laceration repair in the pediatric emergency department. Pediatrics.
2001;26(6):367-74. 2006;117(4):1162-8.
16. Windich-Biermeier A, Sjoberg I, Dale JC, Eshelman D, Guzzetta CE. 33. Sobieraj G, Bhatt M, LeMay S, Rennick J, Johnston C. The effect of
Effects of distraction on pain, fear, and distress during venous port access music on parental participation during pediatric laceration repair. Can J
and venipuncture in children and adolescents with cancer. J Pediatr Nurs Res. 2009;41(4):68-82.
Oncol Nurs. 2007;24(1):8-19. 34. Tanabe P, Ferket K, Thomas R, Paice J, Marcantonio R. The effect of
17. Uman LS, Chambers CT, McGrath PJ, Kisely S. A systematic standard care, ibuprofen, and distraction on pain relief and patient
review of randomized controlled trials examining psychological satisfaction in children with musculoskeletal trauma. J Emerg Nurs.
interventions for needle-related procedural pain and distress in 2002;28(2):118-25.
children and adolescents: an abbreviated Cochrane review. J Pediatr 35. Winskill R, Andrews D. Minimizing the ‘ouch’—a strategy to minimize
Psychol. 2008;33(8):842-54. pain, fear and anxiety in children presenting to the emergency
18. LeMay SS, Johnston C, Choinière M, et al. Pain management department. Australas Emerg Nurs J. 2008;11(4):184-8.
interventions with parents in the emergency department: a randomized 36. Young T, Griffin E, Phillips E, Stanley E. Music as distraction in a
trial. J Advance Nurs. 2010;66(11):2442-9. pediatric emergency department. J Emerg Nurs. 2010;36(5):472-3.
19. O'Donnell J, Maurice SC, Beattie TF. Emergency analgesia in the 37. Curtis SJ, Jou H, Ali S, Vandermeer B, Klassen T. A randomized
paediatric population. Part III non-pharmacological measures of pain controlled trial of sucrose and/or pacifier as analgesia for infants receiving
relief and anxiolysis. Emerg Med J. 2002;19(3):195-7. venipuncture in a pediatric emergency department. Neonatal Intensive
20. Agency for Health Care Policy and Research (AHCPR). Acute Pain Care. 2008;21(3):50.
Management: Operative or 224 Medical Procedures and Trauma. http:// 38. Rogers AJ, Greenwald MH, DeGuzman MA, Kelley ME, Simon HK. A
www.ahrq.gov/clinic/cpgarchv.htm. Published 1992. Accessed Novem- randomized, controlled trial of sucrose analgesia in infants younger than
ber 12, 2010. 90 days of age who require bladder catheterization in the pediatric
21. Bindler R, Ball J, eds. Clinical Skills Manual for Pediatric Nursing: Caring emergency department. Acad Emerg Med. 2006;13(6):617-22.
for Children. 4th ed. New Jersey: Prentice Hall; 2008:98. 39. Acharya A, Annamali S, Taub N, Field D. Oral sucrose analgesia for
22. Wong DL, Baker CM. Pain in children: comparison of assessment preterm infant venipuncture. Arch Dis Child Fetal Neonatal Ed.
scales. Pediatr Nurs. 1988;14(1):9-17. 2004;89:F17-8.
23. Beyer JE, Aradine CR. Content validity of an instrument to measure 40. Herschel M, Khoshnood B, Ellman C, Maydew N, Mittendorf R.
young children's perceptions of the intensity of their pain…the Oucher. Neonatal circumcision. Randomized trial of sucrose pacifier for pain
J Pediatr Nurs. 1986;1(6):386-95. control. Arch Pediatr Adolesc Med. 1998;152(3):279-84.
24. Beyer JE, Aradine CR. Convergent and discriminant validity of a self-report 41. Sparks LA, Setlik J, Luhman J. Parental holding and positioning to
measure of pain intensity for children. Child Health Care. 1988;16(4):274. decrease IV distress in young children: a randomized controlled trial.
25. Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for J Pediatr Nurs. 2007;22(6):440-7.
measurement of acute pain. Acad Emerg Med. 2001;8(12):1153-7. 42. Stephens BK, Barkey ME, Hall HR. Techniques to comfort children
26. Katz E, Kellerman J, Ellenberg L. Hypnosis in the reduction of acute pain during stressful procedures. Adv Mind Body Med. 1999;15(1):49-60.
and distress in children with cancer. J Pediatr Psychol. 1987;12(3):379-94.
27. Carlson KL, Broome M, Vessey JA. Using distraction to reduce reported Submissions to this column are encouraged and may be sent to
pain, fear, and behavioral distress in children and adolescents: a multisite Andrew D. Harding, MS, RN, CEN, NEA-BC, FAHA, FACHE
study. J Soc Pediatr Nurs. 2000;5(2):75-85. ADHardingRN@Gmail.com
150 JOURNAL OF EMERGENCY NURSING VOLUME 39 • ISSUE 2 March 2013
Вам также может понравиться
- Sarcopenia 1Документ2 страницыSarcopenia 1EviОценок пока нет
- Sepsis 2019Документ12 страницSepsis 2019EviОценок пока нет
- Sarcopenia 4Документ7 страницSarcopenia 4EviОценок пока нет
- Early Mobilization For Patient Use Mechanical VentilatorДокумент17 страницEarly Mobilization For Patient Use Mechanical VentilatorEviОценок пока нет
- 10.1371@journal - Pone.0194967 Resiko JatuhДокумент14 страниц10.1371@journal - Pone.0194967 Resiko JatuhEviОценок пока нет
- Vincent2010 SepsisДокумент5 страницVincent2010 SepsisEviОценок пока нет
- Kizilarslanoglu 2016Документ7 страницKizilarslanoglu 2016EviОценок пока нет
- Garnacho Montero2005Документ6 страницGarnacho Montero2005EviОценок пока нет
- Efect of EarlyДокумент12 страницEfect of EarlyEviОценок пока нет
- Vanpee 2014Документ12 страницVanpee 2014EviОценок пока нет
- 2014 BJM MeowsДокумент7 страниц2014 BJM MeowshendraОценок пока нет
- CCM 42 4 2013 09 20 Vanpee 12-02363 SDC1Документ12 страницCCM 42 4 2013 09 20 Vanpee 12-02363 SDC1Roberto Godoy DiazОценок пока нет
- 10 1001@jama 2016 0287Документ10 страниц10 1001@jama 2016 0287ompardor7554Оценок пока нет
- Constitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyДокумент12 страницConstitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyEviОценок пока нет
- Garnacho Montero2005Документ6 страницGarnacho Montero2005EviОценок пока нет
- Vincent2010 SepsisДокумент5 страницVincent2010 SepsisEviОценок пока нет
- Accepted Manuscript: 10.1016/j.chest.2016.10.015Документ56 страницAccepted Manuscript: 10.1016/j.chest.2016.10.015Anonymous 6bOdJC1Оценок пока нет
- Bed Rest and Myopathies: Arny A. Ferrando, Douglas Paddon-Jones and Robert R. WolfeДокумент6 страницBed Rest and Myopathies: Arny A. Ferrando, Douglas Paddon-Jones and Robert R. WolfeEviОценок пока нет
- 10 1001@jama 2016 0287Документ10 страниц10 1001@jama 2016 0287ompardor7554Оценок пока нет
- Constitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyДокумент12 страницConstitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyEviОценок пока нет
- Vincent2010 SepsisДокумент5 страницVincent2010 SepsisEviОценок пока нет
- Aare2013 PDFДокумент9 страницAare2013 PDFEviОценок пока нет
- 10 1001@jama 2016 0287Документ10 страниц10 1001@jama 2016 0287ompardor7554Оценок пока нет
- Intensive Care Unit-Acquired Weakness: Risk Factors and PreventionДокумент7 страницIntensive Care Unit-Acquired Weakness: Risk Factors and PreventionEviОценок пока нет
- Aare2013 PDFДокумент9 страницAare2013 PDFEviОценок пока нет
- 10 1001@jama 2016 0287Документ10 страниц10 1001@jama 2016 0287ompardor7554Оценок пока нет
- Constitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyДокумент12 страницConstitutive Activation of MAPK Cascade in Acute Quadriplegic MyopathyEviОценок пока нет
- 10 1001@jama 2016 0287Документ10 страниц10 1001@jama 2016 0287ompardor7554Оценок пока нет
- Verceles 2018Документ33 страницыVerceles 2018EviОценок пока нет
- Stevens 2007Документ16 страницStevens 2007EviОценок пока нет
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (119)
- Factors Affecting Logistics Performance: A Global Supply Chain PerspectiveДокумент63 страницыFactors Affecting Logistics Performance: A Global Supply Chain PerspectiveAli ArafatОценок пока нет
- Wade Nobles The Intellectual As Healer2Документ17 страницWade Nobles The Intellectual As Healer2Yasmim YonekuraОценок пока нет
- Adventist University MAEd Music EducationДокумент2 страницыAdventist University MAEd Music EducationDorothy FayeОценок пока нет
- Thesis NG Taga PNCДокумент9 страницThesis NG Taga PNCjuliekwhlanchorage100% (2)
- Mathematics Research Paper PDFДокумент7 страницMathematics Research Paper PDFghqmefvhf100% (1)
- Multiple Choice Quiz - Online ResourcesДокумент37 страницMultiple Choice Quiz - Online ResourcesjrenceОценок пока нет
- Chapter 1Документ43 страницыChapter 1Ahmedkan ProofОценок пока нет
- Adorno Authoritarian Personality PDFДокумент314 страницAdorno Authoritarian Personality PDFAlbiHellsing100% (1)
- 978 1 4438 7637 7 SampleДокумент30 страниц978 1 4438 7637 7 SampleSheldon CooperОценок пока нет
- Pantao HS Inset TrainingДокумент7 страницPantao HS Inset TrainingJames LlonaОценок пока нет
- CSR and Brand TrustДокумент79 страницCSR and Brand TrustNagendra Manral100% (2)
- 3.5 Stages of Qualitative ResearchДокумент5 страниц3.5 Stages of Qualitative ResearchSTAR PRINTINGОценок пока нет
- PDF 4Документ9 страницPDF 4api-487657781Оценок пока нет
- Final Report v1.5 LucknowДокумент173 страницыFinal Report v1.5 LucknowED - BankingОценок пока нет
- Education Essay ExamplesДокумент3 страницыEducation Essay Examplescjawrknbf100% (2)
- Heinrich 2013 - State of The Art of Parallel Coordinates PDFДокумент22 страницыHeinrich 2013 - State of The Art of Parallel Coordinates PDFJohОценок пока нет
- TSWJ2014 254932Документ6 страницTSWJ2014 254932khalida iftikharОценок пока нет
- The Art of Asking Essential Questions Based On Critical Thinking Concepts and Socratic Principles byДокумент39 страницThe Art of Asking Essential Questions Based On Critical Thinking Concepts and Socratic Principles byQuang Anh LeОценок пока нет
- Psy 235 Course Outline (U of S)Документ4 страницыPsy 235 Course Outline (U of S)api-290174387Оценок пока нет
- What Is A Research Paper?Документ3 страницыWhat Is A Research Paper?PineappleОценок пока нет
- POA 2 - Effective Risk ManagementДокумент19 страницPOA 2 - Effective Risk ManagementduribotakОценок пока нет
- Accelerating To Impact Project PDFДокумент18 страницAccelerating To Impact Project PDFFirdaus AchmadОценок пока нет
- Vision IAS CSP21T5S CSATДокумент23 страницыVision IAS CSP21T5S CSATamitОценок пока нет
- Simran Kaur FinalДокумент55 страницSimran Kaur FinalDhairya Nagda100% (1)
- Assessment and Control Measures of Flood Risk in Ajibode Area of Ibadan Oyo State NigeriaДокумент16 страницAssessment and Control Measures of Flood Risk in Ajibode Area of Ibadan Oyo State NigeriaArmie SalcedoОценок пока нет
- Impact of Leadership Styles On Employee Performance Case Study of A Non Profit Organization NGO in CambodiaДокумент7 страницImpact of Leadership Styles On Employee Performance Case Study of A Non Profit Organization NGO in CambodiaEditor IJTSRDОценок пока нет
- Prospectus 2013 MT Kenya University KINGDOMДокумент34 страницыProspectus 2013 MT Kenya University KINGDOMJennifer WelchОценок пока нет
- 1 Advertising and Critical Thinking: Unit AimsДокумент12 страниц1 Advertising and Critical Thinking: Unit AimsMA12345Оценок пока нет
- Health Information SystemsДокумент18 страницHealth Information SystemsHanif Gandoh100% (2)
- Original Research Article - Controlling Scabies in Madrasahs (Islamic Religious Schools) in BangladeshДокумент9 страницOriginal Research Article - Controlling Scabies in Madrasahs (Islamic Religious Schools) in BangladeshMuhammad IkbarОценок пока нет