Вам также может понравиться
- Case Study On Observation and Newborn CareДокумент8 страницCase Study On Observation and Newborn CarePiyush Dutta100% (1)
- Kangaroo Mother Care Rooming in UpdatedДокумент44 страницыKangaroo Mother Care Rooming in UpdatedStar DustОценок пока нет
- Needs of New-Born CareДокумент27 страницNeeds of New-Born CarePruthviОценок пока нет
- Case Study On Observation and Newborn CareДокумент38 страницCase Study On Observation and Newborn CarePiyush Dutta100% (2)
- Newborn Care: A Newborn Baby or Animal Is One That Has Just Been BornДокумент26 страницNewborn Care: A Newborn Baby or Animal Is One That Has Just Been BornJenny-Vi Tegelan LandayanОценок пока нет
- Essential Newborn CareДокумент14 страницEssential Newborn CareJam Corros100% (1)
- General Objecti-Wps OfficeДокумент3 страницыGeneral Objecti-Wps OfficeSumit YadavОценок пока нет
- Essential Intrapartum Newborn CareДокумент36 страницEssential Intrapartum Newborn Carefatima chrystelle nuñal100% (1)
- Final PPT - EincДокумент75 страницFinal PPT - EincJia Smith100% (3)
- Seminar On - Essential and Immediate Newborn CareДокумент26 страницSeminar On - Essential and Immediate Newborn CareJyothi Singh SuryavanshiОценок пока нет
- Immediate Newborn Care. BlanksДокумент11 страницImmediate Newborn Care. BlanksMay Princes Torregosa Abucejo100% (1)
- Care NewbornДокумент38 страницCare NewbornRaja0% (1)
- Management of New Born: Presented By: Riya Patel Shukal M.SC (OBGYN)Документ27 страницManagement of New Born: Presented By: Riya Patel Shukal M.SC (OBGYN)BBОценок пока нет
- Essential Intrapartum and Newborn CareДокумент3 страницыEssential Intrapartum and Newborn CareMasterclass40% (5)
- Nursing Care For NewbornДокумент33 страницыNursing Care For NewbornDarla Quiballo100% (1)
- Essential Intrapartum Newborn Care 181120082158 PDFДокумент19 страницEssential Intrapartum Newborn Care 181120082158 PDFDorinna Rizada BagaОценок пока нет
- Infant Care and Feeding Notes 1Документ46 страницInfant Care and Feeding Notes 1Art John CalambaОценок пока нет
- Newborn CareДокумент3 страницыNewborn Careromelisanan848Оценок пока нет
- Assessment of New Born.& Nursing Care of The New Born and Family.Документ14 страницAssessment of New Born.& Nursing Care of The New Born and Family.Manoj TadeОценок пока нет
- EINCДокумент29 страницEINCCelline Isabelle ReyesОценок пока нет
- Management Guideline NICU Updated 2018 - PediMedicineДокумент213 страницManagement Guideline NICU Updated 2018 - PediMedicinenishan chakma100% (1)
- Common Neonatal Problems and Neonatal CareДокумент76 страницCommon Neonatal Problems and Neonatal Caredipali dhayagudeОценок пока нет
- Unit Essential Newborn: 1 CareДокумент29 страницUnit Essential Newborn: 1 CareVijay MgОценок пока нет
- Nursing Care of A Newborn and Family in The Post Partal Period ReviewerДокумент2 страницыNursing Care of A Newborn and Family in The Post Partal Period ReviewerJo PigarОценок пока нет
- Einc-Word 054847Документ4 страницыEinc-Word 054847Jane OrsalОценок пока нет
- Immediate Care of The New Born: ObjectivesДокумент127 страницImmediate Care of The New Born: ObjectivesSwati SharmaОценок пока нет
- FINAL ENC ChecklistДокумент8 страницFINAL ENC ChecklistRaven Torres100% (1)
- Maternal and Child Health Nursing 5 BulletsДокумент5 страницMaternal and Child Health Nursing 5 BulletsHoneylie PatricioОценок пока нет
- NCM 104 Lec Reviewer FinalsДокумент11 страницNCM 104 Lec Reviewer FinalsFERNANDEZ, RELLY ANDREWОценок пока нет
- EINC Essential Intrapartim NC ChecklistДокумент7 страницEINC Essential Intrapartim NC Checklisthey aadarshaОценок пока нет
- Essential Newborn Care Protocol: Warsame, Ahmed Sebanes, Kimberky Mae Silao, Emee JoyДокумент35 страницEssential Newborn Care Protocol: Warsame, Ahmed Sebanes, Kimberky Mae Silao, Emee JoyKathlyn SunicoОценок пока нет
- BHW TRAINING Newborn HealthДокумент24 страницыBHW TRAINING Newborn HealthWilma BeraldeОценок пока нет
- Care of NewornДокумент4 страницыCare of NewornArchana SahuОценок пока нет
- I. View The Science and Art of Breastfeeding VO815 and Putting It All Into Practice V0816 On The Ground Floor Computer LabДокумент11 страницI. View The Science and Art of Breastfeeding VO815 and Putting It All Into Practice V0816 On The Ground Floor Computer Lablec06cОценок пока нет
- Unang YakapДокумент57 страницUnang YakapHelen Grace Avila100% (3)
- Neonatal NursingДокумент53 страницыNeonatal Nursingkrishnasree100% (1)
- Teaching ProgramДокумент6 страницTeaching ProgramLizly Letrondo-PinoteОценок пока нет
- Nursing Care of Newborn and FamilyДокумент38 страницNursing Care of Newborn and FamilyLady Jane CaguladaОценок пока нет
- Nursing Care of A Neonate Part 1Документ67 страницNursing Care of A Neonate Part 1Rani G SОценок пока нет
- DR Guide 1Документ49 страницDR Guide 1Alyza ElisesОценок пока нет
- Einc G5Документ24 страницыEinc G5JAMIL MANALОценок пока нет
- Fix Care of NewbornДокумент39 страницFix Care of Newborngratzia fionaОценок пока нет
- BREASTFEEDINGДокумент19 страницBREASTFEEDINGIsmael JaaniОценок пока нет
- Module Essential Newborn CareДокумент26 страницModule Essential Newborn CareMichtropolisОценок пока нет
- Med Surg 2 BulletsДокумент19 страницMed Surg 2 BulletsShiraishiОценок пока нет
- Essential Newborn CareДокумент20 страницEssential Newborn Carejanjan_cepilloОценок пока нет
- Routine New Born Care GNMДокумент55 страницRoutine New Born Care GNMLeena Pravil100% (3)
- Unang YakapДокумент3 страницыUnang YakapBernadeth Labrador100% (1)
- DLPДокумент3 страницыDLPKathrina AlfonsoОценок пока нет
- of Newborn CareДокумент42 страницыof Newborn CareGurpreet kaur100% (9)
- Die Poor Weight Gain: Cesarean SectionДокумент4 страницыDie Poor Weight Gain: Cesarean SectionYoussef AliОценок пока нет
- EINC Essential Intrapartim NC ChecklistДокумент7 страницEINC Essential Intrapartim NC ChecklistNur Fatima SanaaniОценок пока нет
- Umbilical Infection in Newborns: Newborn Care SeriesДокумент3 страницыUmbilical Infection in Newborns: Newborn Care Serieszelvininaprilia990Оценок пока нет
- EINCДокумент50 страницEINC1S - FERNANDEZ, KRISTELLE LOUISE I.Оценок пока нет
- EENC (Early Essential Newborn Care)Документ74 страницыEENC (Early Essential Newborn Care)Jennifer AlamonОценок пока нет
- Essential Intrapartum and Newborn CareДокумент5 страницEssential Intrapartum and Newborn Careanjie kamidОценок пока нет
- RD Manual Med and BathingДокумент5 страницRD Manual Med and Bathingapple m.Оценок пока нет
- Unang YakapДокумент9 страницUnang YakapWeng Maesa MontemayorОценок пока нет
- Respiratory - Distress (1) 2 PDFДокумент8 страницRespiratory - Distress (1) 2 PDFSatya Prakash TiwariОценок пока нет
- Neonatalresuscitationmanual2 PDFДокумент75 страницNeonatalresuscitationmanual2 PDFSatya Prakash TiwariОценок пока нет
- HypothermiaДокумент5 страницHypothermiaMRS CHAKRAPANIОценок пока нет
- Respiratory - Distress (1) 2 PDFДокумент8 страницRespiratory - Distress (1) 2 PDFSatya Prakash TiwariОценок пока нет
- Equipment Demonstration: National Neonatology ForumДокумент53 страницыEquipment Demonstration: National Neonatology ForumSatya Prakash TiwariОценок пока нет
- Neonataljaundice PDFДокумент7 страницNeonataljaundice PDFSatya Prakash TiwariОценок пока нет
- Breastfeeding PDFДокумент11 страницBreastfeeding PDFSatya Prakash TiwariОценок пока нет
- Fluid Management: Learning ObjectivesДокумент6 страницFluid Management: Learning ObjectivesSatya Prakash TiwariОценок пока нет
- Neonatal Seizures: Learning ObjectivesДокумент6 страницNeonatal Seizures: Learning ObjectivesSatya Prakash TiwariОценок пока нет
- Neonatal Sepsis: Learning ObjectivesДокумент10 страницNeonatal Sepsis: Learning ObjectivesSatya Prakash TiwariОценок пока нет
- NRP PDFДокумент6 страницNRP PDFSatya Prakash TiwariОценок пока нет
- HypothermiaДокумент5 страницHypothermiaMRS CHAKRAPANIОценок пока нет
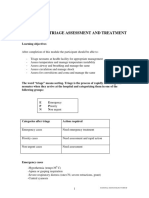
- Emergency Triage Assessment and Treatment: National Neonatology ForumДокумент6 страницEmergency Triage Assessment and Treatment: National Neonatology ForumSatya Prakash TiwariОценок пока нет
- Umbilical Cord ProlapseДокумент5 страницUmbilical Cord Prolapseangga hergaОценок пока нет
- Umbilical Cord Blood Bank, Future Child Health InsuranceДокумент2 страницыUmbilical Cord Blood Bank, Future Child Health Insurancenvtaa rnaОценок пока нет
- Blood Gas AnalysisДокумент5 страницBlood Gas AnalysisPathrecia Natalia SiagianОценок пока нет
- Ped CL April2015Документ244 страницыPed CL April2015JOAQUIN PEDRE100% (1)
- Advanced Neonatal Procedure1Документ14 страницAdvanced Neonatal Procedure1Santhosh.S.U100% (1)
- Placenta Umbilical CordДокумент39 страницPlacenta Umbilical Cordbel4ronaldoeОценок пока нет
- IFC Core CompetencyДокумент7 страницIFC Core CompetencyLloyd Rafael EstabilloОценок пока нет
- Pierre BudinДокумент3 страницыPierre BudinFer45Оценок пока нет
- 4 Anatomy of The Ductus Venosus in Neonatal Dogs (Canis Familiaris)Документ4 страницы4 Anatomy of The Ductus Venosus in Neonatal Dogs (Canis Familiaris)ValeriaMolinaCanoОценок пока нет
- 1642 CompressedДокумент246 страниц1642 CompressedJasonZambranoRojasОценок пока нет
- Placenta ExaminationДокумент2 страницыPlacenta ExaminationSumit YadavОценок пока нет
- Newborn Assessment: By: Ledelle M. de Chavez, Claudine M. Francisco & Don Jayric V. DepalobosДокумент5 страницNewborn Assessment: By: Ledelle M. de Chavez, Claudine M. Francisco & Don Jayric V. Depalobosdonskii04Оценок пока нет
- Internship ReportДокумент42 страницыInternship ReportSunil S GowdaОценок пока нет
- Section: General ObstetricsДокумент15 страницSection: General ObstetricsvarmaОценок пока нет
- Immediate Newborn CareДокумент5 страницImmediate Newborn CareHannah Angelu Cabading50% (2)
- Social Banking Agreement - Pan India (Retail) - 23-08-2018Документ11 страницSocial Banking Agreement - Pan India (Retail) - 23-08-2018Rajat KaushikОценок пока нет
- The Prevalence and Risk Factors For Hyperbilirubinemia in NeonatesДокумент4 страницыThe Prevalence and Risk Factors For Hyperbilirubinemia in NeonatesIJAR JOURNALОценок пока нет
- Stem Cell Cryobank: Cord Blood and Stem Cells For LifeДокумент23 страницыStem Cell Cryobank: Cord Blood and Stem Cells For LifelyndonlinОценок пока нет
- Ob Evaluation 1 Final - Sec AДокумент33 страницыOb Evaluation 1 Final - Sec AKarla Mae Israel CamarintaОценок пока нет
- Obladen 2010Документ7 страницObladen 2010Barna ÉvaОценок пока нет
- Ready 0903Документ6 страницReady 0903sylvianapfОценок пока нет
- Maternal and Child Health Nursing (NCM 101 Lect) Part 1Документ4 страницыMaternal and Child Health Nursing (NCM 101 Lect) Part 1yunjung0518100% (7)
- Test Bank For Comprehensive Perinatal and Pediatric Respiratory Care 4th Edition by Whitaker Isbn 10 1439059438 Isbn 13 9781439059432Документ7 страницTest Bank For Comprehensive Perinatal and Pediatric Respiratory Care 4th Edition by Whitaker Isbn 10 1439059438 Isbn 13 9781439059432trangdatif0Оценок пока нет
- قياس بعض المعادن الثقيلة في دم الحبل السري لحديثي الولادة وأمهاتهم PDFДокумент221 страницаقياس بعض المعادن الثقيلة في دم الحبل السري لحديثي الولادة وأمهاتهم PDFSalam H Alhelali0% (1)
- Clear My Choice: Not Yet Answered Marked Out of 1.00Документ7 страницClear My Choice: Not Yet Answered Marked Out of 1.00medodiabОценок пока нет
- Need For More Evidence in The Prevention and Management of PerinatalДокумент10 страницNeed For More Evidence in The Prevention and Management of PerinatalNATALY HASTAMORY VANEGASОценок пока нет
- DR Guide 1Документ49 страницDR Guide 1Alyza ElisesОценок пока нет
- URACHUSДокумент10 страницURACHUStikarosandaliОценок пока нет
- PEDIA Nursing NCLEX Bullets Part 1Документ166 страницPEDIA Nursing NCLEX Bullets Part 1Russel Myron Adriano AdvinculaОценок пока нет
- A Pre Experimental Study To Assess The Effectiveness of STP On Knowledge Regarding Umbilical Cord Blood Banking Among Nursing Students at Selected Areas in JammuДокумент6 страницA Pre Experimental Study To Assess The Effectiveness of STP On Knowledge Regarding Umbilical Cord Blood Banking Among Nursing Students at Selected Areas in JammuEditor IJTSRDОценок пока нет
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОт EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsОценок пока нет
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisОт EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisРейтинг: 4.5 из 5 звезд4.5/5 (42)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeОт EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeРейтинг: 2 из 5 звезд2/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsОт EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsРейтинг: 5 из 5 звезд5/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityОт EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityРейтинг: 4 из 5 звезд4/5 (24)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedОт EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedРейтинг: 5 из 5 звезд5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossОт EverandThe Obesity Code: Unlocking the Secrets of Weight LossРейтинг: 4 из 5 звезд4/5 (6)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaОт EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsОт EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsРейтинг: 4.5 из 5 звезд4.5/5 (169)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDОт EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDРейтинг: 5 из 5 звезд5/5 (1)
- Why We Die: The New Science of Aging and the Quest for ImmortalityОт EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityРейтинг: 4 из 5 звезд4/5 (3)
- Gut: the new and revised Sunday Times bestsellerОт EverandGut: the new and revised Sunday Times bestsellerРейтинг: 4 из 5 звезд4/5 (392)
- The Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeОт EverandThe Courage Habit: How to Accept Your Fears, Release the Past, and Live Your Courageous LifeРейтинг: 4.5 из 5 звезд4.5/5 (253)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsОт EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsРейтинг: 3.5 из 5 звезд3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisОт EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisРейтинг: 3.5 из 5 звезд3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningОт EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningРейтинг: 4 из 5 звезд4/5 (3)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.От EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Рейтинг: 4.5 из 5 звезд4.5/5 (110)
- To Explain the World: The Discovery of Modern ScienceОт EverandTo Explain the World: The Discovery of Modern ScienceРейтинг: 3.5 из 5 звезд3.5/5 (51)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessОт EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessРейтинг: 4.5 из 5 звезд4.5/5 (328)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisОт EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (1)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryОт EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryРейтинг: 4 из 5 звезд4/5 (44)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)