Вам также может понравиться
- Preclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1От EverandPreclinical Behavioral Science and Social Sciences Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Оценок пока нет
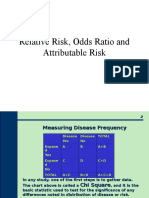
- Or RR PressentationДокумент13 страницOr RR PressentationredityoОценок пока нет
- Spatial TB AnalysisДокумент16 страницSpatial TB AnalysisCristóbal GarcíaОценок пока нет
- Who - Bulletin VN PrevalenceДокумент8 страницWho - Bulletin VN PrevalenceNguyen Binh HoaОценок пока нет
- Risk TBДокумент13 страницRisk TBM Caesar NovaldyОценок пока нет
- 2010 UNAIDS Global ReportДокумент46 страниц2010 UNAIDS Global ReportImperator FuriosaОценок пока нет
- TB in MyanmarДокумент6 страницTB in MyanmarMichael KhaОценок пока нет
- EpidemiologyДокумент21 страницаEpidemiologyNadia ShadОценок пока нет
- Pedoman KomentarДокумент6 страницPedoman KomentarDimas MeetОценок пока нет
- Prevalence Ratio in CrossДокумент3 страницыPrevalence Ratio in CrossAlmira Shabrina SaraswatiОценок пока нет
- Predicting The Unpredictable: Transmission of Drug-Resistant HIVДокумент5 страницPredicting The Unpredictable: Transmission of Drug-Resistant HIVCarlos Alfredo Ramirez PeñaОценок пока нет
- 6.2 More Times Than ReportedДокумент12 страниц6.2 More Times Than ReportedMahmoudAboAlSamenОценок пока нет
- Frequency Measures: Morbidity: Classical Epidemiology 623Документ41 страницаFrequency Measures: Morbidity: Classical Epidemiology 623Mayson BaliОценок пока нет
- Estimating The True Prevalence of Mycobacterium Bovis in Hunter-Harvested White-Tailed Deer in MichiganДокумент11 страницEstimating The True Prevalence of Mycobacterium Bovis in Hunter-Harvested White-Tailed Deer in MichiganHartarto AkhmadОценок пока нет
- Measurement of Diseases - LmaДокумент35 страницMeasurement of Diseases - LmaLim Wei EnОценок пока нет
- Risk factors incidence prevalence rates epidemiologyДокумент30 страницRisk factors incidence prevalence rates epidemiologyWafaa AdamОценок пока нет
- SSRN Id3635047Документ93 страницыSSRN Id3635047cgeacarОценок пока нет
- Infectious Diseases Epidemiology and ModellingДокумент39 страницInfectious Diseases Epidemiology and ModellingLeonel NkwetiОценок пока нет
- Measurementofdisease FinalДокумент79 страницMeasurementofdisease Finalbiniam yohannesОценок пока нет
- Incidence and Prevalence PDFДокумент9 страницIncidence and Prevalence PDFSreya SanilОценок пока нет
- La Carga de La Enfermedad de Chagas Estimaciones y Desafios Stanawal 2015Документ6 страницLa Carga de La Enfermedad de Chagas Estimaciones y Desafios Stanawal 2015Adriana Santander OliveraОценок пока нет
- Statistics: Why Do We Measure ?: Nazmus Saquib Ph.D. Associate Professor Sulaiman Al-Rajhi UniversityДокумент29 страницStatistics: Why Do We Measure ?: Nazmus Saquib Ph.D. Associate Professor Sulaiman Al-Rajhi UniversityANAN ALSURAYYIОценок пока нет
- Alexandria D. - Illinois US (2019) - RuralДокумент8 страницAlexandria D. - Illinois US (2019) - RuralIVAN ANGEL HUAMANI LINARESОценок пока нет
- Environmental Epidemiology: AbbreviationsДокумент9 страницEnvironmental Epidemiology: AbbreviationsOsbelОценок пока нет
- Epidemiology Lab ManualДокумент34 страницыEpidemiology Lab ManualDominique SmithОценок пока нет
- Keaslian 3 Di PakaiДокумент10 страницKeaslian 3 Di PakaiAfraОценок пока нет
- HIV and AIDS where is the epidemic goingДокумент9 страницHIV and AIDS where is the epidemic going1w3r5y7i9p10qpОценок пока нет
- 1 - Mathematical Formulation of Hepatitis B Virus With Optimal Control Analysis PDFДокумент16 страниц1 - Mathematical Formulation of Hepatitis B Virus With Optimal Control Analysis PDFindah rania729Оценок пока нет
- Epidemiology of Tuberculosis in USAДокумент10 страницEpidemiology of Tuberculosis in USALeo AcОценок пока нет
- Chapter 3 Measures of Disease Frequency, Copy Copy CopyДокумент43 страницыChapter 3 Measures of Disease Frequency, Copy Copy CopyEstiv W. StigОценок пока нет
- 2-3basic Measurments in EpidemiologyДокумент6 страниц2-3basic Measurments in EpidemiologyalhashemisaqrОценок пока нет
- Upward Trend in Hospitalized Dengue Cases in the United StatesДокумент6 страницUpward Trend in Hospitalized Dengue Cases in the United StatesArhaMozaОценок пока нет
- JTLD 27 03 10 - 1..8Документ9 страницJTLD 27 03 10 - 1..8Reixel Raquel MugruzaОценок пока нет
- Tuberculosis InfectionДокумент17 страницTuberculosis Infectionkib240309Оценок пока нет
- Com - MS - Seshadri - 11-18july2020 - Pages 14-17Документ4 страницыCom - MS - Seshadri - 11-18july2020 - Pages 14-17Arushi SinghОценок пока нет
- The Global HIV/AIDS Epidemic: Key FactsДокумент9 страницThe Global HIV/AIDS Epidemic: Key Factsvhina valerieОценок пока нет
- Intensity of Exposure To Pulmonary Tuberculosis Determines Risk of Tuberculosis Infection and DiseaseДокумент10 страницIntensity of Exposure To Pulmonary Tuberculosis Determines Risk of Tuberculosis Infection and DiseaseYu YuОценок пока нет
- Ecological Niche Modeling of West Nile Virus Transmission Potential in Kent County, Michigan - Frimodig, WingДокумент29 страницEcological Niche Modeling of West Nile Virus Transmission Potential in Kent County, Michigan - Frimodig, WingKendall FrimodigОценок пока нет
- TB ReportДокумент7 страницTB ReporthennyОценок пока нет
- Late Diagnosis of Hiv Infection in Iaşi County - Frequency, Associated Factors, Therapeutic OptionsДокумент5 страницLate Diagnosis of Hiv Infection in Iaşi County - Frequency, Associated Factors, Therapeutic OptionsVata LuminitaОценок пока нет
- Bennett Et Al-2008Документ8 страницBennett Et Al-2008fatimakh462Оценок пока нет
- HIV in Colombia: An Epidemiologic Point of ViewДокумент8 страницHIV in Colombia: An Epidemiologic Point of ViewJuanJoseHerreraBerrioОценок пока нет
- TB Overview FactsheetДокумент3 страницыTB Overview FactsheetGavinОценок пока нет
- Tambo, Adetunde and Olalubi 2018 PDFДокумент7 страницTambo, Adetunde and Olalubi 2018 PDFOluwasegun AdetundeОценок пока нет
- Global Numbers of Infection and Disease Burden of Soil Transmitted Helminth Infections in 2010Документ19 страницGlobal Numbers of Infection and Disease Burden of Soil Transmitted Helminth Infections in 2010Yuanita ClaraОценок пока нет
- Tuberculosis Contact Investigations - United States, 2003-2012Документ24 страницыTuberculosis Contact Investigations - United States, 2003-2012viannikkkyОценок пока нет
- Tropmed 91 1002Документ9 страницTropmed 91 1002Khalifah Future LearningОценок пока нет
- MM 5940Документ32 страницыMM 5940worksheetbookОценок пока нет
- Health Environtment Measures - DR - SiswantoДокумент43 страницыHealth Environtment Measures - DR - Siswantoseptian kristyanaОценок пока нет
- Measure of The DiseaseДокумент13 страницMeasure of The DiseaseGhada ElhassanОценок пока нет
- Epidemiology - Definitions of TermsДокумент3 страницыEpidemiology - Definitions of Termsali_mumtajОценок пока нет
- Measures of MorbidityДокумент46 страницMeasures of Morbidityadarsh hegdeОценок пока нет
- Sexually Transmitted Diseases Among American Youth: Incidence and Prevalence Estimates, 2000Документ5 страницSexually Transmitted Diseases Among American Youth: Incidence and Prevalence Estimates, 2000Amalia nurlailyОценок пока нет
- CommunityViralLoadinHIV PDFДокумент9 страницCommunityViralLoadinHIV PDFIsaias PrestesОценок пока нет
- National Estimate of HIV Seroprevalence Among Tuberculosis Patients in IndiaДокумент3 страницыNational Estimate of HIV Seroprevalence Among Tuberculosis Patients in IndianutheadОценок пока нет
- Measures of Disease Frequency NOTESДокумент22 страницыMeasures of Disease Frequency NOTESSJ JungОценок пока нет
- 79 (12) 1121 1132Документ15 страниц79 (12) 1121 1132rispanОценок пока нет
- Ototoksis KanamicynДокумент20 страницOtotoksis KanamicynFarhan Rizqy RОценок пока нет
- Hepatology - 2004 - Alter - Epidemiology of Hepatitis CДокумент4 страницыHepatology - 2004 - Alter - Epidemiology of Hepatitis CEngr Hafiz Qasim AliОценок пока нет
- Measuring Risk, Incidence - Prevalence (Practical)Документ6 страницMeasuring Risk, Incidence - Prevalence (Practical)kyomuhendobright4Оценок пока нет
- Oral Bacteria and Bowel Diseases Mini Review 2161 069X 1000404Документ4 страницыOral Bacteria and Bowel Diseases Mini Review 2161 069X 1000404kib240309Оценок пока нет
- MH ScreeningChartДокумент22 страницыMH ScreeningChartkib240309Оценок пока нет
- 1 s2.0 S1684118219300726 MainДокумент7 страниц1 s2.0 S1684118219300726 Mainkib240309Оценок пока нет
- Mapping Field Data on Google MapsДокумент11 страницMapping Field Data on Google Mapskib240309Оценок пока нет
- Oxidative Stress Mechanisms and Their Modulation PDFДокумент183 страницыOxidative Stress Mechanisms and Their Modulation PDFkib240309Оценок пока нет
- Contribution of The Collagen-Binding Proteins of Streptococcus Mutans To Bacterial Colonization of Inflamed Dental PulpДокумент13 страницContribution of The Collagen-Binding Proteins of Streptococcus Mutans To Bacterial Colonization of Inflamed Dental Pulpkib240309Оценок пока нет
- SxceДокумент13 страницSxceicaeeeОценок пока нет
- Screening DiABEES Mnc03Документ54 страницыScreening DiABEES Mnc03Deepu SebinОценок пока нет
- NuropathologyДокумент1 страницаNuropathologykib240309Оценок пока нет
- Frequently Asked QuestionsДокумент3 страницыFrequently Asked Questionskib240309Оценок пока нет
- Frequently Asked QuestionsДокумент3 страницыFrequently Asked Questionskib240309Оценок пока нет
- RenalДокумент19 страницRenalkib240309Оценок пока нет
- Tuberculosis InfectionДокумент17 страницTuberculosis Infectionkib240309Оценок пока нет
- Frequently Asked QuestionsДокумент3 страницыFrequently Asked Questionskib240309Оценок пока нет
- Summary of MH Screening and Assessment Tools For Primary CareДокумент20 страницSummary of MH Screening and Assessment Tools For Primary CareTeresa Meehan100% (1)
- BursitisДокумент5 страницBursitiskib240309Оценок пока нет
- H & E ProtocolДокумент1 страницаH & E ProtocolAdeel SarfrazОценок пока нет
- Emergency SonographyДокумент1 страницаEmergency Sonographykib240309Оценок пока нет
- This Sample Document May Not Conform To The Standards of Your Local Research Ethics BoardДокумент7 страницThis Sample Document May Not Conform To The Standards of Your Local Research Ethics Boardkib240309Оценок пока нет
- Stem Cell Research GuidelinesДокумент5 страницStem Cell Research Guidelineskib240309Оценок пока нет
- Pediatric RadiologyДокумент7 страницPediatric Radiologykib240309Оценок пока нет
- Stem CellДокумент2 страницыStem Cellkib240309Оценок пока нет
- CoreДокумент1 страницаCorekib240309Оценок пока нет
- CPS BC STI Treatment Guidelines 20112014Документ11 страницCPS BC STI Treatment Guidelines 20112014Maria Teresa SanromanОценок пока нет
- Tuansi-Pa ManuscriptДокумент11 страницTuansi-Pa Manuscriptallkhusairy6tuansiОценок пока нет
- Parasitology PresentationДокумент28 страницParasitology PresentationSamuel WilliamsОценок пока нет
- 61cb1a364d1a3e4a04bee5bb - Employee Wellness PlanДокумент25 страниц61cb1a364d1a3e4a04bee5bb - Employee Wellness PlanDigvijay KadamОценок пока нет
- Prinsip Dan Teori Kesehatan Masyarakat: Mohamad Guntur Nangi, Skm.,M.KesДокумент35 страницPrinsip Dan Teori Kesehatan Masyarakat: Mohamad Guntur Nangi, Skm.,M.KesvanesaОценок пока нет
- Drug StudyДокумент8 страницDrug StudyJoel MadjosОценок пока нет
- The Corset and It's ReputationДокумент10 страницThe Corset and It's ReputationElleanna Gasparevic0% (1)
- Nbme 29 Questions (200) Done 211Документ200 страницNbme 29 Questions (200) Done 211Shahzeen Sajid KhanОценок пока нет
- Biobank Doggo - Purpose - Partnership - and - Possibilities - The - ImplemenДокумент11 страницBiobank Doggo - Purpose - Partnership - and - Possibilities - The - ImplemenTri4alОценок пока нет
- Compilation Questions of Theory Part One 04-1Документ34 страницыCompilation Questions of Theory Part One 04-1Rebecca WongОценок пока нет
- Cardiac Case Study Homework Week 5Документ4 страницыCardiac Case Study Homework Week 5Study AssistantОценок пока нет
- 2020NSDUHFFR1PDFW102121Документ156 страниц2020NSDUHFFR1PDFW102121bachillerataОценок пока нет
- Molar PregnancyДокумент13 страницMolar PregnancyShalynurОценок пока нет
- Anterior Canal BPPV and Apogeotropic PosteriorДокумент9 страницAnterior Canal BPPV and Apogeotropic PosteriorRudolfGerОценок пока нет
- Sancho Vs AbellaДокумент2 страницыSancho Vs Abellajerico kier nonoОценок пока нет
- Dental Caries Vaccine ExplainedДокумент30 страницDental Caries Vaccine Explainedpublic health health svsidsОценок пока нет
- 3 Introduction 10.12Документ10 страниц3 Introduction 10.12Barbie QueОценок пока нет
- Buku Biopsi InterpretationДокумент552 страницыBuku Biopsi InterpretationelisasitohangОценок пока нет
- Neuro-Ophthalmology Review Provides Insight into Optic Nerve DisordersДокумент48 страницNeuro-Ophthalmology Review Provides Insight into Optic Nerve DisordersJL BillsОценок пока нет
- 1A Silvestre, Ped - Tuberculosis ModuleДокумент8 страниц1A Silvestre, Ped - Tuberculosis ModulePed SilvestreОценок пока нет
- Hemolytic AnemiaДокумент18 страницHemolytic AnemiabryankekОценок пока нет
- HP MatsuhisaДокумент11 страницHP MatsuhisaGantuya BoldbaatarОценок пока нет
- Physical Fitness Components: Mr. Edward Ryan V. AyalaДокумент32 страницыPhysical Fitness Components: Mr. Edward Ryan V. AyalaShina Mae Abellera Barrameda100% (1)
- Miglamin Es Learning Continuity PlanДокумент33 страницыMiglamin Es Learning Continuity PlancherryОценок пока нет
- Drug-Study OmeprazoleДокумент1 страницаDrug-Study OmeprazoleBeverly Datu71% (7)
- Res 113Документ197 страницRes 113Belinda ELISHAОценок пока нет
- Twelve Tips To Leverage AI For Efficient and Effective Medical Question Generation A Guide For Educators Using Chat GPTДокумент7 страницTwelve Tips To Leverage AI For Efficient and Effective Medical Question Generation A Guide For Educators Using Chat GPTÇağla ErgönenОценок пока нет
- How Soon Can You Drink Alcohol After Getting Your Covid-19 Vaccine - SA Corona Virus Online PortalДокумент1 страницаHow Soon Can You Drink Alcohol After Getting Your Covid-19 Vaccine - SA Corona Virus Online PortalArjay GudoyОценок пока нет
- Reading 4 - Avk43 - Online - Version 2Документ7 страницReading 4 - Avk43 - Online - Version 2Kim ChâuОценок пока нет
- Nicolas Ortner The Tapping Solution EFTДокумент17 страницNicolas Ortner The Tapping Solution EFTBambang Prasetyo100% (2)