Вам также может понравиться
- 3 Neonatal InfectionДокумент56 страниц3 Neonatal InfectiondindaamalaОценок пока нет
- Neonatal InfectionДокумент56 страницNeonatal InfectionGanesha Gamma 2017Оценок пока нет
- Neonatal InfectionДокумент56 страницNeonatal InfectionAgust SalimОценок пока нет
- Neonatal Infection: Julniar M Tasli Herman Bermawi Afifa RamadantiДокумент56 страницNeonatal Infection: Julniar M Tasli Herman Bermawi Afifa RamadantiOtchi Pudtrie WijayaОценок пока нет
- Neonatal InfectionДокумент56 страницNeonatal InfectionajengdwintaОценок пока нет
- Neonatal Sepsis: Dr. Sunil Kumar Yadav MBBS, MD, DM NeonatologyДокумент64 страницыNeonatal Sepsis: Dr. Sunil Kumar Yadav MBBS, MD, DM NeonatologyKulgaurav RegmiОценок пока нет
- Neonatal SepsisДокумент7 страницNeonatal Sepsispaningbatan.kristine.bОценок пока нет
- Neonatal Sepsis 2019.Документ6 страницNeonatal Sepsis 2019.Jean Paúl LópezОценок пока нет
- Neonatal Sepsis 2018Документ40 страницNeonatal Sepsis 2018Abraham AnaelyОценок пока нет
- Neonatal SepsisДокумент38 страницNeonatal SepsisJavier Saad100% (1)
- Kırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisДокумент40 страницKırşehir Ahi Evran Üniversitesi Sağlık Bilimleri Enstitüsü: Neonatal Sepsis & MeningitisAli FalihОценок пока нет
- Neonatal Bacterial InfectionДокумент8 страницNeonatal Bacterial InfectionNuurОценок пока нет
- Immunization in Child: Dr. MD Gde Dwi Lingga Utama, Sp.A (K) Dr. I Wayan Gustawan, MSC., Spa (K) Department of Child HealthДокумент58 страницImmunization in Child: Dr. MD Gde Dwi Lingga Utama, Sp.A (K) Dr. I Wayan Gustawan, MSC., Spa (K) Department of Child HealthgabriellafelisaОценок пока нет
- Sepsis in Newborns (Flores, Christine Mae & Espiritu, Richelle)Документ9 страницSepsis in Newborns (Flores, Christine Mae & Espiritu, Richelle)Carlojay IniegoОценок пока нет
- Neonatal Meningitis: Designed By: Dr. Esraa AlnabilsyДокумент19 страницNeonatal Meningitis: Designed By: Dr. Esraa AlnabilsyAli FalihОценок пока нет
- Newborn and Infant Conditions GuideДокумент4 страницыNewborn and Infant Conditions GuideYuuki Chitose (tai-kun)Оценок пока нет
- Neonatal Sepsis & MeningitisДокумент39 страницNeonatal Sepsis & MeningitisIbrahimОценок пока нет
- Dr. Omnictin's guide to infectious diseases in pregnancyДокумент15 страницDr. Omnictin's guide to infectious diseases in pregnancyroselo alagaseОценок пока нет
- Kuliah Mahasiswan UPH, Neonatal SepsisДокумент39 страницKuliah Mahasiswan UPH, Neonatal Sepsiswilliam atmadjiОценок пока нет
- Neonatal Meningitis, The Facts: Key PointsДокумент4 страницыNeonatal Meningitis, The Facts: Key PointsSanjeev GargОценок пока нет
- Neonatal SepsisДокумент51 страницаNeonatal SepsisAngelo Del VentoОценок пока нет
- PEDIATRIC NURSING IIIДокумент3 страницыPEDIATRIC NURSING IIIRizalyn Padua ReyОценок пока нет
- Neonatal Sepsis 5-09 ModifiedДокумент39 страницNeonatal Sepsis 5-09 ModifiedAbraham AnaelyОценок пока нет
- Neonatal Sepsis 1219225703095484 9Документ50 страницNeonatal Sepsis 1219225703095484 9Ali FalihОценок пока нет
- SepsisДокумент17 страницSepsiswizborrlyzo006Оценок пока нет
- Immunization Schedule for Infants and ChildrenДокумент50 страницImmunization Schedule for Infants and ChildrenElaine Frances IlloОценок пока нет
- Neonatal SepsisДокумент63 страницыNeonatal SepsisDemewoz Fikir100% (2)
- Puerperal SepsisДокумент4 страницыPuerperal SepsisSonali NayakОценок пока нет
- Neonatal InfectionsДокумент41 страницаNeonatal Infectionsamid sultanОценок пока нет
- Meningitis (Completed)Документ26 страницMeningitis (Completed)seema83% (6)
- Neonatal SepsisДокумент6 страницNeonatal SepsisSunaina AdhikariОценок пока нет
- Neonatal Sepsis and Necrotizing EnterocolitisДокумент47 страницNeonatal Sepsis and Necrotizing EnterocolitisAljeirou AlcachupasОценок пока нет
- Neonatal Meningitis, The Facts: Key PointsДокумент4 страницыNeonatal Meningitis, The Facts: Key PointsSatria RachmatОценок пока нет
- Sumu PDFДокумент30 страницSumu PDFalokpalreshaОценок пока нет
- Detect Neonatal Sepsis EarlyДокумент102 страницыDetect Neonatal Sepsis EarlygcezcurraОценок пока нет
- Neonatal Meningitis, The Facts: Key PointsДокумент4 страницыNeonatal Meningitis, The Facts: Key PointsDenisa RotaruОценок пока нет
- Neonatal Meningitis, The Facts: Key PointsДокумент4 страницыNeonatal Meningitis, The Facts: Key PointsDenisa RotaruОценок пока нет
- Identification and classification of infections in neonatesДокумент62 страницыIdentification and classification of infections in neonatesvisuinsvu100% (7)
- Newborn DisordersIДокумент23 страницыNewborn DisordersInicewanОценок пока нет
- Gomella - SepsisДокумент15 страницGomella - SepsisJustine Frances CabalayОценок пока нет
- Neonatal Sepsis Case StudyДокумент6 страницNeonatal Sepsis Case StudyCatherine PradoОценок пока нет
- 10 - Torch Pads KehamilanДокумент43 страницы10 - Torch Pads KehamilanMuhammad LutfiОценок пока нет
- NEONATAL INFECTIONS: CAUSES, SIGNS AND TREATMENTДокумент86 страницNEONATAL INFECTIONS: CAUSES, SIGNS AND TREATMENTSanjay Kumar SanjuОценок пока нет
- Livret MF GB21Документ20 страницLivret MF GB21mary15eugОценок пока нет
- Immunization and VaccinesДокумент21 страницаImmunization and VaccinesMaiga Ayub HusseinОценок пока нет
- Pola Imunologi Janin Dalam Kehamilan Dengan Toxoplasmosis: Khairunnisa Abd Rauf A.Zakaria Amien Octo ZulkarnainДокумент18 страницPola Imunologi Janin Dalam Kehamilan Dengan Toxoplasmosis: Khairunnisa Abd Rauf A.Zakaria Amien Octo ZulkarnainArdian Zaka RAОценок пока нет
- Vaccination Principles & ImmunityДокумент27 страницVaccination Principles & ImmunityReynaldiSanjayaОценок пока нет
- Infectia Cu CMVДокумент31 страницаInfectia Cu CMVminerva_stanciuОценок пока нет
- Immunological Aspect of Immunization: Dr. Rahmawati Minhajat, PH.D, SP - PDДокумент31 страницаImmunological Aspect of Immunization: Dr. Rahmawati Minhajat, PH.D, SP - PDNurul fatimahОценок пока нет
- Toxoplasmosis in PregnancyДокумент45 страницToxoplasmosis in PregnancyTahta PambudiОценок пока нет
- Neonatal SepsisДокумент33 страницыNeonatal SepsisDharma Danny FernsОценок пока нет
- Immunity & Principles of VaccinationДокумент27 страницImmunity & Principles of VaccinationAniruddha RoyОценок пока нет
- PDF INFECTIOUS and INFLAMMATORYДокумент51 страницаPDF INFECTIOUS and INFLAMMATORYRivera CharmaineОценок пока нет
- VaccinationДокумент28 страницVaccinationM AQIB ASLAMОценок пока нет
- MS Semifinals Complete NotesДокумент59 страницMS Semifinals Complete NotesMarvie TorralbaОценок пока нет
- SepsisДокумент3 страницыSepsisronzenrocker02Оценок пока нет
- Abnormal PuerperiumДокумент23 страницыAbnormal Puerperiumseema pundirОценок пока нет
- Lecture - Immunization and VaccinesДокумент40 страницLecture - Immunization and Vaccinesrockyrawat01012003Оценок пока нет
- Female Urinary Tract Infections in Clinical PracticeОт EverandFemale Urinary Tract Infections in Clinical PracticeBob YangОценок пока нет
- 9.insulin Treatment in ChildДокумент21 страница9.insulin Treatment in Childirene aureliaОценок пока нет
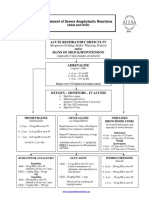
- AnaphylacticДокумент1 страницаAnaphylacticirene aureliaОценок пока нет
- Who His HWF Amr 2018.1 EngДокумент28 страницWho His HWF Amr 2018.1 EngMaulina ManurungОценок пока нет
- Bedolla Barajas2018Документ7 страницBedolla Barajas2018irene aureliaОценок пока нет
- 1240-Article Text-2900-1-10-20170201 PDFДокумент7 страниц1240-Article Text-2900-1-10-20170201 PDFirene aureliaОценок пока нет
- Peters2018 PDFДокумент10 страницPeters2018 PDFirene aureliaОценок пока нет
- Vitamin D Status in Egyptian Children With Allergic RhinitisДокумент5 страницVitamin D Status in Egyptian Children With Allergic Rhinitisirene aureliaОценок пока нет
- Can 2018Документ4 страницыCan 2018Ayiek WicaksonoОценок пока нет
- Heart Murmurs in Healthy Newborn Babies 28.0.011Документ3 страницыHeart Murmurs in Healthy Newborn Babies 28.0.011constantinОценок пока нет
- Transport of Sick NB PDFДокумент25 страницTransport of Sick NB PDFirene aurelia100% (1)
- Vitamin D Status in Egyptian Children With Allergic RhinitisДокумент5 страницVitamin D Status in Egyptian Children With Allergic Rhinitisirene aureliaОценок пока нет
- Walsh 2018Документ3 страницыWalsh 2018irene aureliaОценок пока нет
- 13.sick Day Management in CHДокумент12 страниц13.sick Day Management in CHirene aureliaОценок пока нет
- 9.insulin Treatment in ChildДокумент21 страница9.insulin Treatment in Childirene aureliaОценок пока нет
- Multisite NIRS Application Precourse Arend BosДокумент39 страницMultisite NIRS Application Precourse Arend Bosirene aureliaОценок пока нет
- Peters2018 PDFДокумент10 страницPeters2018 PDFirene aureliaОценок пока нет
- Association Between Caesarean Delivery and Isolated Doses of Formula Feeding in Cow Milk AllergyДокумент6 страницAssociation Between Caesarean Delivery and Isolated Doses of Formula Feeding in Cow Milk Allergyirene aureliaОценок пока нет
- Rina Ramayani Komplikasi SN KONIKA XVIIДокумент26 страницRina Ramayani Komplikasi SN KONIKA XVIIirene aureliaОценок пока нет
- Neonatal Transport - Diane CoadДокумент28 страницNeonatal Transport - Diane Coadirene aureliaОценок пока нет
- Transport of Sick NB PDFДокумент25 страницTransport of Sick NB PDFirene aurelia100% (1)
- Initial Assessment On PresentationДокумент2 страницыInitial Assessment On PresentationAnggita Dewi RahmasariОценок пока нет
- 1692-Article Text-4776-1-10-20180308 PDFДокумент6 страниц1692-Article Text-4776-1-10-20180308 PDFirene aureliaОценок пока нет
- Rtc-Scent 2012 05 Octaplex ProtocolДокумент1 страницаRtc-Scent 2012 05 Octaplex Protocolirene aureliaОценок пока нет
- HIV - Aids Lecture DR Nabil.1Документ25 страницHIV - Aids Lecture DR Nabil.1Hannan AliОценок пока нет
- Open Letter English 2010 AssignmentДокумент5 страницOpen Letter English 2010 Assignmentapi-551077399Оценок пока нет
- OUTBREAK RESEARCH: AFRICAN SLEEPING SICKNESSДокумент10 страницOUTBREAK RESEARCH: AFRICAN SLEEPING SICKNESSDuncan DaoОценок пока нет
- Epi NotesДокумент5 страницEpi NoteshoneykrizelОценок пока нет
- History of MedivineДокумент39 страницHistory of Medivinelionking68Оценок пока нет
- CarmelliДокумент5 страницCarmellinana PrimasantiОценок пока нет
- Cutaneous Larva MigransДокумент4 страницыCutaneous Larva MigransanissabilfaqihОценок пока нет
- The Economics of Conspiracy TheoriesДокумент8 страницThe Economics of Conspiracy Theorieszadanliran100% (1)
- CA AdrenalДокумент8 страницCA AdrenalCleysser Antonio Custodio PolarОценок пока нет
- Microorganisms in Kitchen SpongesДокумент6 страницMicroorganisms in Kitchen SpongesYami SainzОценок пока нет
- Acupressure Points To Treat Swelling&EdemaДокумент11 страницAcupressure Points To Treat Swelling&EdemabmomeraliОценок пока нет
- Lymph NodesДокумент6 страницLymph NodesIsak ShatikaОценок пока нет
- DangueДокумент2 страницыDangueJeetesh RathiОценок пока нет
- Chronic Lateral Ankle PainДокумент6 страницChronic Lateral Ankle PainLetchumanan L MarimuthuОценок пока нет
- MDHHS Legionnaires EmailsДокумент53 страницыMDHHS Legionnaires EmailsClickon DetroitОценок пока нет
- Cryptosporidium Key FactsДокумент5 страницCryptosporidium Key Factsalang_businessОценок пока нет
- Kimberley Dodd Assignment 2b RaftДокумент7 страницKimberley Dodd Assignment 2b Raftapi-239323495Оценок пока нет
- What Is Bronchitis? Symptoms, Causes, TreatmentДокумент1 страницаWhat Is Bronchitis? Symptoms, Causes, TreatmentMelvin Lopez SilvestreОценок пока нет
- The History of Visayan Village: Tagum City'S Most Populated BarangayДокумент11 страницThe History of Visayan Village: Tagum City'S Most Populated BarangayJay Jay JayyiОценок пока нет
- Listening and Speaking Book - 11 Elite & 12 Advanced - Chapter 6 Healthy Mind, Healthy BodyДокумент20 страницListening and Speaking Book - 11 Elite & 12 Advanced - Chapter 6 Healthy Mind, Healthy BodySue JaОценок пока нет
- NACO - National Technical Guidelines On ART - October 2018 PDFДокумент282 страницыNACO - National Technical Guidelines On ART - October 2018 PDFPriyamboda Mohanty (SAATHII)Оценок пока нет
- Colon's Role in Chronic ArthritisДокумент5 страницColon's Role in Chronic ArthritisIG0% (1)
- Visually Impaired PresentationДокумент11 страницVisually Impaired PresentationRajesh SoniОценок пока нет
- Microorganisms' Beneficial Role in Food IndustryДокумент3 страницыMicroorganisms' Beneficial Role in Food IndustryLady Quinte MОценок пока нет
- Tinea PedisДокумент4 страницыTinea PediskirustagyОценок пока нет
- WHO Malaria Elimination - A Field ManualДокумент98 страницWHO Malaria Elimination - A Field ManualMacAbc100% (3)
- Definition of PneumoniaДокумент4 страницыDefinition of PneumoniaEmylia Ananda PutriОценок пока нет
- Communicative II, Unit 2 QuestionsДокумент2 страницыCommunicative II, Unit 2 QuestionsAddis VLOG100% (3)
- Contoh Soal Announcement Text Dan JawabanДокумент6 страницContoh Soal Announcement Text Dan JawabanItha Hernita Novianti100% (1)
- Physical Distancing, Face MaskДокумент16 страницPhysical Distancing, Face MaskshdudvegОценок пока нет