Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- Candidate Handbook For State Credentialing: For The National Counselor ExaminationДокумент13 страницCandidate Handbook For State Credentialing: For The National Counselor ExaminationHec ChavezОценок пока нет
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- 2 MMPI-2 Validity-Scales Final PDFДокумент9 страниц2 MMPI-2 Validity-Scales Final PDFHanifa Bi BaritoОценок пока нет
- Candidate Handbook For State Credentialing: For The National Counselor ExaminationДокумент13 страницCandidate Handbook For State Credentialing: For The National Counselor ExaminationHec ChavezОценок пока нет
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Candidate Handbook For State Credentialing: For The National Counselor ExaminationДокумент13 страницCandidate Handbook For State Credentialing: For The National Counselor ExaminationHec ChavezОценок пока нет
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- C A N SДокумент111 страницC A N SHec ChavezОценок пока нет
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Self Care WheelДокумент1 страницаSelf Care Wheelapi-356243627100% (3)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Taking ActionДокумент120 страницTaking ActionHec ChavezОценок пока нет
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Vicarious Resilience: A New Concept in Work With Those Who Survive TraumaДокумент15 страницVicarious Resilience: A New Concept in Work With Those Who Survive TraumaHec ChavezОценок пока нет
- Self Care WheelДокумент1 страницаSelf Care Wheelapi-356243627100% (3)
- Boundaries in TherapyДокумент2 страницыBoundaries in TherapyHec ChavezОценок пока нет
- Social PhobiaДокумент128 страницSocial PhobiaAhmad Arif Ramli67% (3)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Self CareДокумент3 страницыSelf CareHec ChavezОценок пока нет
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- Identifying Associations Among Co-Occurring Medical Conditions in Children With Autism Spectrum DisordersДокумент7 страницIdentifying Associations Among Co-Occurring Medical Conditions in Children With Autism Spectrum DisordersHec ChavezОценок пока нет
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- AU StudiesДокумент6 страницAU StudiesHec ChavezОценок пока нет
- Identifying Associations Among Co-Occurring Medical Conditions in Children With Autism Spectrum DisordersДокумент7 страницIdentifying Associations Among Co-Occurring Medical Conditions in Children With Autism Spectrum DisordersHec ChavezОценок пока нет
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Research ETДокумент15 страницResearch ETHec ChavezОценок пока нет
- Treatment Patterns in Children With Autism in The United StatesДокумент10 страницTreatment Patterns in Children With Autism in The United StatesHec ChavezОценок пока нет
- Autism and Young Children - Painting A Picture For Nevada PDFДокумент11 страницAutism and Young Children - Painting A Picture For Nevada PDFHec ChavezОценок пока нет
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- Autism and Young Children - Painting A Picture For Nevada PDFДокумент11 страницAutism and Young Children - Painting A Picture For Nevada PDFHec ChavezОценок пока нет
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- Treatment of Elopement Without Blocking With A Child With AutismДокумент14 страницTreatment of Elopement Without Blocking With A Child With AutismHec ChavezОценок пока нет
- AU TreatmentДокумент6 страницAU TreatmentHec ChavezОценок пока нет
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- AU StudiesДокумент6 страницAU StudiesHec ChavezОценок пока нет
- CoachingДокумент15 страницCoachingHec ChavezОценок пока нет
- Treatment Patterns in Children With Autism in The United StatesДокумент10 страницTreatment Patterns in Children With Autism in The United StatesHec ChavezОценок пока нет
- AAMFT Code of Ethics PDFДокумент10 страницAAMFT Code of Ethics PDFHec ChavezОценок пока нет
- Treatment of Elopement Without Blocking With A Child With AutismДокумент14 страницTreatment of Elopement Without Blocking With A Child With AutismHec ChavezОценок пока нет
- Cognitive-Behavioral Group Therapy For Intermittent Explosive Disorder: Description and Preliminary AnalysisДокумент4 страницыCognitive-Behavioral Group Therapy For Intermittent Explosive Disorder: Description and Preliminary AnalysisHec ChavezОценок пока нет
- Bsi 18Документ10 страницBsi 18Ismael RonnyОценок пока нет
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Is Path WarmДокумент2 страницыIs Path WarmDANIELОценок пока нет
- Medication Card CelebrexДокумент2 страницыMedication Card CelebrexTSPAN100% (1)
- Ebook - Yoga - The Science of BreathДокумент2 страницыEbook - Yoga - The Science of BreathGabriel CiocanОценок пока нет
- 2023 Aaha Senior Care Guidelines For Dogs and CatsДокумент21 страница2023 Aaha Senior Care Guidelines For Dogs and CatsisvpОценок пока нет
- Source: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical EthicsДокумент67 страницSource: Bioethics Topics: Exam Questions & Answers Legal Medicine & Medical Ethicsjamestery0% (1)
- Phytochemical Screening and Extraction A ReviewДокумент9 страницPhytochemical Screening and Extraction A Reviewsaivasya50% (2)
- 2015 Case 6 MBUДокумент12 страниц2015 Case 6 MBUDinesh TiwariОценок пока нет
- A New Lingual Straight-Wire Techique: Journal of Clinical Orthodontics: JCO February 2010Документ11 страницA New Lingual Straight-Wire Techique: Journal of Clinical Orthodontics: JCO February 2010Hafaifa TaiebОценок пока нет
- Pemanfaatan Teknik Assisted Hatching Dalam Meningkatkan Implantasi EmbrioДокумент10 страницPemanfaatan Teknik Assisted Hatching Dalam Meningkatkan Implantasi EmbrioMumutTeaОценок пока нет
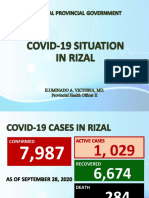
- Covid19 Situation in RizalДокумент23 страницыCovid19 Situation in RizalToni Quitalig GamezОценок пока нет
- EDIC Guidelines 2017 PDFДокумент22 страницыEDIC Guidelines 2017 PDFZia ShaikhОценок пока нет
- Anti Psychotic DrugsДокумент2 страницыAnti Psychotic DrugsJohn Corpuz100% (1)
- Jsa For Complete Erection of Tank-001Документ52 страницыJsa For Complete Erection of Tank-001Ashutosh80% (10)
- Procalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsДокумент2 страницыProcalcitonin Testing To Guide Antibiotic Therapy in Acute Upper and Lower Respiratory Tract InfectionsMr. LОценок пока нет
- Parkinsons Presentation Case StudyДокумент33 страницыParkinsons Presentation Case Studyapi-287759747Оценок пока нет
- Article - CVD Cardiac Arrest - Bls AclsДокумент2 страницыArticle - CVD Cardiac Arrest - Bls AclsAkhosh SomarajanОценок пока нет
- Aseptic MeningitisДокумент24 страницыAseptic Meningitisidno1008100% (1)
- Information Technology in SurgeryДокумент38 страницInformation Technology in Surgerydooshy50% (4)
- Lactated Ringer'sДокумент7 страницLactated Ringer'sPPLaloОценок пока нет
- D. Santhi Krupa, Et Al IJAPRДокумент6 страницD. Santhi Krupa, Et Al IJAPRAtraoОценок пока нет
- Windy WigaДокумент2 страницыWindy WigaWindy wigaОценок пока нет
- Mental Health ActДокумент48 страницMental Health ActGursabeen KalraОценок пока нет
- (2012) - Psychosis and GenderДокумент2 страницы(2012) - Psychosis and GenderChoko DelgadoОценок пока нет
- Prescription - Apollo 2471688806157843Документ2 страницыPrescription - Apollo 2471688806157843shahidliftsОценок пока нет
- OrthopedicДокумент1 страницаOrthopedicapi-352507025Оценок пока нет
- The 25 PROTOCOL: Important Exercise For SciaticaДокумент8 страницThe 25 PROTOCOL: Important Exercise For SciaticaDr Ahmed NabilОценок пока нет
- Burnout: From Popular Culture To Psychiatric Diagnosis in SwedenДокумент21 страницаBurnout: From Popular Culture To Psychiatric Diagnosis in SwedenRajan PandaОценок пока нет
- Massage TherapyДокумент79 страницMassage TherapyMukesh Duryodhan Hirekhan100% (1)
- Tissue TypingДокумент4 страницыTissue TypingNoura Al-Hussainan100% (1)
- Sources of Homeopathic DrugsДокумент35 страницSources of Homeopathic Drugsnadiida83% (6)
- The Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeОт EverandThe Upward Spiral: Using Neuroscience to Reverse the Course of Depression, One Small Change at a TimeРейтинг: 4.5 из 5 звезд4.5/5 (140)
- Summary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDОт EverandSummary of The Body Keeps the Score: Brain, Mind, and Body in the Healing of Trauma by Bessel van der Kolk MDРейтинг: 4.5 из 5 звезд4.5/5 (167)
- Summary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisОт EverandSummary: The Myth of Normal: Trauma, Illness, and Healing in a Toxic Culture By Gabor Maté MD & Daniel Maté: Key Takeaways, Summary & AnalysisРейтинг: 4 из 5 звезд4/5 (9)
- Rewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryОт EverandRewire Your Anxious Brain: How to Use the Neuroscience of Fear to End Anxiety, Panic, and WorryРейтинг: 4.5 из 5 звезд4.5/5 (157)