Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Dingenen 2017Документ14 страницDingenen 2017pedro.coleffОценок пока нет
- Outback MenuДокумент2 страницыOutback MenuzeeОценок пока нет
- Leadership 29Документ32 страницыLeadership 29Efe AgbozeroОценок пока нет
- Cell Division-Mitosis Notes: 2 New CellsДокумент21 страницаCell Division-Mitosis Notes: 2 New CellsCristina MariaОценок пока нет
- Entomotherapy, or The Medicinal Use of InsectsДокумент23 страницыEntomotherapy, or The Medicinal Use of InsectsJessica Revelo OrdoñezОценок пока нет
- Jurnal Kasus Etikolegal Dalam Praktik KebidananДокумент13 страницJurnal Kasus Etikolegal Dalam Praktik KebidananErni AnggieОценок пока нет
- Supplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11Документ81 страницаSupplementary Spec To API Specification 17D Subsea Wellhead and Tree Equipment With Justifications S 561Jv2022 11maximusala83Оценок пока нет
- Telecommunications GroundingДокумент24 страницыTelecommunications GroundingMike FordealsОценок пока нет
- 10.4324 9781315717289 PreviewpdfДокумент179 страниц10.4324 9781315717289 PreviewpdfMahdi GargouriОценок пока нет
- Conference Proceedings: Inhaled Nitric Oxide: Delivery Systems and MonitoringДокумент27 страницConference Proceedings: Inhaled Nitric Oxide: Delivery Systems and MonitoringPhanОценок пока нет
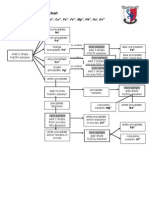
- Testing For Cations Flow ChartДокумент2 страницыTesting For Cations Flow Chartapi-252561013Оценок пока нет
- Megapower: Electrosurgical GeneratorДокумент45 страницMegapower: Electrosurgical GeneratorAnibal Alfaro VillatoroОценок пока нет
- Leader Ship Assessment: Student No 374212036Документ4 страницыLeader Ship Assessment: Student No 374212036Emily KimОценок пока нет
- Different Types of FermentationДокумент26 страницDifferent Types of FermentationCats and DogОценок пока нет
- NABARD Grade A 2020 Phase 2 ESI ARDДокумент6 страницNABARD Grade A 2020 Phase 2 ESI ARDrohit bhosadОценок пока нет
- Chinese Cinderella - MeДокумент2 страницыChinese Cinderella - Meapi-298120057100% (1)
- Stern TubesДокумент8 страницStern Tubesweesweekwee8652Оценок пока нет
- Fitting in and Fighting Back: Stigma Management Strategies Among Homeless KidsДокумент24 страницыFitting in and Fighting Back: Stigma Management Strategies Among Homeless KidsIrisha AnandОценок пока нет
- World Wide Emission Free E-Motercycle ProjectДокумент20 страницWorld Wide Emission Free E-Motercycle ProjectAkshay SharmaОценок пока нет
- Afcat Question Paper 01-2014 PDFДокумент10 страницAfcat Question Paper 01-2014 PDFTuhin AzadОценок пока нет
- History of Crime and Criminal Justice in America EditedДокумент7 страницHistory of Crime and Criminal Justice in America EditedcarolineОценок пока нет
- Book Summary - I Hear You Summary Michael Sorensen - Read in 7 MinutesДокумент10 страницBook Summary - I Hear You Summary Michael Sorensen - Read in 7 MinutesNogüey JoseОценок пока нет
- User Manual 4372070Документ80 страницUser Manual 4372070EDENILSON CORDEIROОценок пока нет
- Final Workshop Report On Value Addition and AgroprocessingДокумент31 страницаFinal Workshop Report On Value Addition and AgroprocessingBett K. BernardОценок пока нет
- ENT Head and Neck ExamДокумент21 страницаENT Head and Neck ExamvickyОценок пока нет
- Leoline Installation and MaintenanceДокумент8 страницLeoline Installation and MaintenanceFloorkitОценок пока нет
- AcuityPDR BrochureДокумент3 страницыAcuityPDR BrochureJulian HutabaratОценок пока нет
- Bars Performance AppraisalДокумент6 страницBars Performance AppraisalPhillip Miler0% (1)
- Soal Uh English XДокумент1 страницаSoal Uh English XhenniherawatiОценок пока нет
- How Hydraulic Valve Lifters WorkДокумент1 страницаHow Hydraulic Valve Lifters WorkSanket Sabale100% (1)