Вам также может понравиться
- Level of Exposure To Childhood Tuberculosis in Household Contacts With Adult Pulmonary TuberculosisДокумент6 страницLevel of Exposure To Childhood Tuberculosis in Household Contacts With Adult Pulmonary Tuberculosisdapajiangu asniОценок пока нет
- Mendeley 03Документ5 страницMendeley 03faraОценок пока нет
- 43-Article Text-117-1-10-20200210Документ11 страниц43-Article Text-117-1-10-20200210ChacongsОценок пока нет
- Youth Perspective On Pulmonary Tuberculosis Parent's CareДокумент7 страницYouth Perspective On Pulmonary Tuberculosis Parent's CareIJPHSОценок пока нет
- Wurzel 2016Документ8 страницWurzel 2016prolanis pkmmulyoharjoОценок пока нет
- Risk Factor TuberculinДокумент7 страницRisk Factor TuberculinAnonymous oUg5v1p4zОценок пока нет
- Ajol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204Документ6 страницAjol File Journals - 494 - Articles - 112516 - Submission - Proof - 112516 5833 312396 1 10 20150204ASK De OliveiraОценок пока нет
- 259-Article Text-998-1-10-20191127 PDFДокумент12 страниц259-Article Text-998-1-10-20191127 PDFyayahОценок пока нет
- Pencabutan Ventilator Journal ReadingДокумент19 страницPencabutan Ventilator Journal ReadingzainОценок пока нет
- BMJ c4978 FullДокумент6 страницBMJ c4978 Fulljesusm_115Оценок пока нет
- Infants Hospitalized For Bordetella Pertussis Infection Commonly Have Respiratory Viral CoinfectionsДокумент6 страницInfants Hospitalized For Bordetella Pertussis Infection Commonly Have Respiratory Viral CoinfectionsYuscha AnindyaОценок пока нет
- Tuberculosis in Children Exposed at Home To MultidrugДокумент12 страницTuberculosis in Children Exposed at Home To MultidrugElsa HasibuanОценок пока нет
- Paediatrica Indonesiana: Clarissa Cita Magdalena, Budi Utomo, Retno Asih SetyoningrumДокумент7 страницPaediatrica Indonesiana: Clarissa Cita Magdalena, Budi Utomo, Retno Asih SetyoningrumputerinmОценок пока нет
- As Ma Pediatric AДокумент6 страницAs Ma Pediatric APatricia GuíoОценок пока нет
- Cep 2020 00339Документ23 страницыCep 2020 00339Elison J PanggaloОценок пока нет
- TB AnakДокумент6 страницTB AnakHerlin Ajeng NurrahmaОценок пока нет
- Hubungan Riwayat Kontak Penderita Tuberkulosis Paru (TB) Dengan Kejadian TB Paru Anak Di Balai Pengobatan Penyakit Paru-Paru (Bp4) PurwokertoДокумент6 страницHubungan Riwayat Kontak Penderita Tuberkulosis Paru (TB) Dengan Kejadian TB Paru Anak Di Balai Pengobatan Penyakit Paru-Paru (Bp4) PurwokertoIra TryОценок пока нет
- Community-Acquired Pneumonia in Children: Myths and FactsДокумент4 страницыCommunity-Acquired Pneumonia in Children: Myths and FactsFranciscoDelgadoОценок пока нет
- Literature ToddlerДокумент4 страницыLiterature ToddlerValarmathiОценок пока нет
- 7 Mira 64 - 79Документ16 страниц7 Mira 64 - 79Faizal Rezza FahlefiОценок пока нет
- Extensively Drug-Resistant Tuberculosis in Children With HumanДокумент12 страницExtensively Drug-Resistant Tuberculosis in Children With Humanromeoenny4154Оценок пока нет
- Neumonia Por InfluenzaДокумент19 страницNeumonia Por InfluenzaEdgar GavilanesОценок пока нет
- ZNJ - Volume 17 - Issue 2 - Pages 1-13Документ13 страницZNJ - Volume 17 - Issue 2 - Pages 1-13Ljc JaslinОценок пока нет
- 12701-50629-1-PB-1 AnakДокумент4 страницы12701-50629-1-PB-1 AnakAni RoseОценок пока нет
- Risk Factors for Childhood TuberculosisДокумент5 страницRisk Factors for Childhood TuberculosisAnthony Huaman MedinaОценок пока нет
- Adiutarini 2Документ7 страницAdiutarini 2Eva Tirtabayu HasriОценок пока нет
- Factors Linked to Childhood Pulmonary TB CasesДокумент16 страницFactors Linked to Childhood Pulmonary TB CasesNafik MunaОценок пока нет
- Nama:Rohaninda Nim.:18.030 Tugas Resume:Bahasa Inggris Medical JournalДокумент15 страницNama:Rohaninda Nim.:18.030 Tugas Resume:Bahasa Inggris Medical JournalNhynda ParaniОценок пока нет
- Probiotics and Carriage of Streptococcus PneumoniaeДокумент9 страницProbiotics and Carriage of Streptococcus Pneumoniaeanita awОценок пока нет
- Articulo 1Документ6 страницArticulo 1Esteban Jose Hernandez ZotoОценок пока нет
- 335 Full PDFДокумент7 страниц335 Full PDFcrsscribdОценок пока нет
- Community Acquired Pneumonia in ChildrenДокумент62 страницыCommunity Acquired Pneumonia in ChildrenThea DinoОценок пока нет
- E20161309 FullДокумент12 страницE20161309 Fullwajarsi pratamiОценок пока нет
- Tdap Vaccine Effectiveness in Adolescents (Acosta 2017)Документ11 страницTdap Vaccine Effectiveness in Adolescents (Acosta 2017)gd_hbarОценок пока нет
- Jean Retrospective Analysis of Candida-Related Conditions in Childhood Cari SyO9CZhДокумент5 страницJean Retrospective Analysis of Candida-Related Conditions in Childhood Cari SyO9CZhIrsalina SalmaОценок пока нет
- 4000 11827 1 SMДокумент11 страниц4000 11827 1 SMJulia Gustina sariОценок пока нет
- Association Between Nutritional Status and Severity of Pneumonia Among Children Under Five Years Attending Wangaya District HospitalДокумент7 страницAssociation Between Nutritional Status and Severity of Pneumonia Among Children Under Five Years Attending Wangaya District HospitalchairulОценок пока нет
- Clinical and Demographic Profile of Pediatric Patients With Dengue Fever Admitted in Three Hospitals in Tagbilaran City 2161 0665 1000332Документ6 страницClinical and Demographic Profile of Pediatric Patients With Dengue Fever Admitted in Three Hospitals in Tagbilaran City 2161 0665 1000332nailaОценок пока нет
- 08 0119 PDFДокумент8 страниц08 0119 PDFAnailil MoralesОценок пока нет
- First Line FluДокумент6 страницFirst Line Flu419022 MELA ANANDA PUTRIANAОценок пока нет
- Idr 7 153 PDFДокумент13 страницIdr 7 153 PDFwubet birhanОценок пока нет
- Astma1 Jurnal ReadingДокумент10 страницAstma1 Jurnal ReadingRizki NabilaОценок пока нет
- Diagnosis of Pneumonia in Children With Dehydrating DiarrhoeaДокумент6 страницDiagnosis of Pneumonia in Children With Dehydrating DiarrhoeaEmaa AmooraОценок пока нет
- Ni Kadek Ethi Yudiastuti, Anak Agung Sagung Sawitri, Dewa Nyoman WirawanДокумент7 страницNi Kadek Ethi Yudiastuti, Anak Agung Sagung Sawitri, Dewa Nyoman WirawanRabiatulAОценок пока нет
- Pneumonia Clinical Case Study BSN 2 2 Group 4Документ43 страницыPneumonia Clinical Case Study BSN 2 2 Group 4Precious Jenichris TamayoОценок пока нет
- Probiotics and Child Care Absence Due To Infections: A Randomized Controlled TrialДокумент11 страницProbiotics and Child Care Absence Due To Infections: A Randomized Controlled TrialMuhammad FebrianОценок пока нет
- Usia TBДокумент9 страницUsia TBViviОценок пока нет
- A Community-Based Isoniazid Preventive Therapy For PDFДокумент8 страницA Community-Based Isoniazid Preventive Therapy For PDFbekele badeОценок пока нет
- NIH Public Access: Author ManuscriptДокумент17 страницNIH Public Access: Author ManuscriptAndika ZuldiansyahОценок пока нет
- Journal Reading VH 1Документ4 страницыJournal Reading VH 1richard 102017193Оценок пока нет
- Jurnal TB (Anak)Документ6 страницJurnal TB (Anak)Hakim Abdul PakayaОценок пока нет
- Childhood Asthma Is Associated With Development of Type 1 Diabetes and Inflammatory Bowel Diseases: A Danish Nationwide Registry StudyДокумент9 страницChildhood Asthma Is Associated With Development of Type 1 Diabetes and Inflammatory Bowel Diseases: A Danish Nationwide Registry Studykholoud mohamedОценок пока нет
- 1 s2.0 S0929664616302480 MainДокумент9 страниц1 s2.0 S0929664616302480 MainEniola JayeolaОценок пока нет
- Fped 09 599500Документ8 страницFped 09 599500Safira SalsabilaОценок пока нет
- Trend and Outcome of Sepsis in ChildrenДокумент8 страницTrend and Outcome of Sepsis in ChildrenGunduz AgaОценок пока нет
- Pulmonary Tuberculosis in Children: Maryam Keshtkar Jahromi Batool Sharifi-MoodДокумент4 страницыPulmonary Tuberculosis in Children: Maryam Keshtkar Jahromi Batool Sharifi-MoodRositaadlОценок пока нет
- The Definition of Pneumonia, The Assessment of Severity, and Clinical Standardization in The Pneumonia Etiology Research For Child Health StudyДокумент8 страницThe Definition of Pneumonia, The Assessment of Severity, and Clinical Standardization in The Pneumonia Etiology Research For Child Health StudyHusseini ElghamryОценок пока нет
- JCDR 10 LC08Документ6 страницJCDR 10 LC08kurniawan martОценок пока нет
- Treating The Wheezing Infant: Ronina A. Covar, MD, Joseph D. Spahn, MDДокумент24 страницыTreating The Wheezing Infant: Ronina A. Covar, MD, Joseph D. Spahn, MDSophia RoseОценок пока нет
- In the Shadow of Illness: Parents and Siblings of the Chronically Ill ChildОт EverandIn the Shadow of Illness: Parents and Siblings of the Chronically Ill ChildОценок пока нет
- Anthropometry of The Scapula - Clinical and Surgical ConsiderationsДокумент8 страницAnthropometry of The Scapula - Clinical and Surgical ConsiderationsAdam JohnsonОценок пока нет
- Anthropometric Study of The Proximal Radius - Does Radial Head Implant Fit in All CasesДокумент9 страницAnthropometric Study of The Proximal Radius - Does Radial Head Implant Fit in All CasesAdam JohnsonОценок пока нет
- Rrtherhic Chethrthtynjhyttt I 2011Документ11 страницRrtherhic Chethrthtynjhyttt I 2011Adam JohnsonОценок пока нет
- Bahan 1Документ40 страницBahan 1Adam JohnsonОценок пока нет
- Bahan 2Документ25 страницBahan 2Adam JohnsonОценок пока нет
- Osteogenesis Imperfecta: New Perspectives From Clinical and Translational ResearchДокумент10 страницOsteogenesis Imperfecta: New Perspectives From Clinical and Translational ResearchAdam JohnsonОценок пока нет
- Good PDFДокумент6 страницGood PDFAdam JohnsonОценок пока нет
- Bahan 3Документ11 страницBahan 3Adam JohnsonОценок пока нет
- Current Concepts in Osteogenesis Imperfecta - Bone Structure, Biomechanics and Medical ManagementДокумент11 страницCurrent Concepts in Osteogenesis Imperfecta - Bone Structure, Biomechanics and Medical ManagementDennisFrankKondoОценок пока нет
- Nitric Oxide: SciencedirectДокумент9 страницNitric Oxide: SciencedirectAdam JohnsonОценок пока нет
- Best Practice & Research Clinical AnaesthesiologyДокумент10 страницBest Practice & Research Clinical AnaesthesiologyAdam JohnsonОценок пока нет
- 1 s2.0 S1043661816306697 MainДокумент13 страниц1 s2.0 S1043661816306697 MainAdam JohnsonОценок пока нет
- 09-Chandran Et AlДокумент6 страниц09-Chandran Et AlAdam JohnsonОценок пока нет
- Review Article: Mouse Fracture Models: A PrimerДокумент12 страницReview Article: Mouse Fracture Models: A PrimerAdam JohnsonОценок пока нет
- 5481 21722 1 PB PDFДокумент5 страниц5481 21722 1 PB PDFAdam JohnsonОценок пока нет
- Non Union of Fracture Neck of Femur For Intertrochanteric OsteotomyДокумент4 страницыNon Union of Fracture Neck of Femur For Intertrochanteric OsteotomyAdam JohnsonОценок пока нет
- Influence of Age On Mechanical Properties of Healing Fractures and Intact Bones in RatsДокумент9 страницInfluence of Age On Mechanical Properties of Healing Fractures and Intact Bones in RatsAdam JohnsonОценок пока нет
- Cirugia Periodontal Manejo Recesiones Gingivales en 1 o Mas DiengtesДокумент21 страницаCirugia Periodontal Manejo Recesiones Gingivales en 1 o Mas DiengtesAlejandro MorenoОценок пока нет
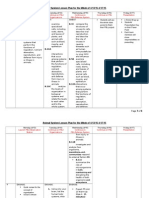
- Animal System Lesson PlanДокумент6 страницAnimal System Lesson Planapi-266567690Оценок пока нет
- Request for Medical or Religious Exemption from Flu VaccineДокумент1 страницаRequest for Medical or Religious Exemption from Flu Vaccineplayboi501Оценок пока нет
- Burton's Microbiology Ch1Документ38 страницBurton's Microbiology Ch1Carl Elexer Cuyugan Ano91% (11)
- Family Nursing Care PlanДокумент3 страницыFamily Nursing Care PlanColleen De la Rosa100% (1)
- Juvenile Idiopathic Arthritis TypesДокумент1 страницаJuvenile Idiopathic Arthritis TypesDinesh ReddyОценок пока нет
- CHN Ii 1-100Документ12 страницCHN Ii 1-100Yanna JaucianОценок пока нет
- SMC CompiledДокумент2 страницыSMC CompiledLovely De CastroОценок пока нет
- Chapter 20 HomeworkДокумент9 страницChapter 20 HomeworkKvn4N6Оценок пока нет
- Trifold BrochureДокумент2 страницыTrifold BrochureRendanLumbertОценок пока нет
- Mycoses: Mallare - Morales - QuibalДокумент67 страницMycoses: Mallare - Morales - QuibalBianca MoralesОценок пока нет
- Soal Uts Bahasa Inggris JBДокумент6 страницSoal Uts Bahasa Inggris JB21081010302 Moh. Ayyuhan FawwazansaОценок пока нет
- General Santos City Hospitals and Healthcare FacilitiesДокумент25 страницGeneral Santos City Hospitals and Healthcare FacilitiesVeronica HendrickОценок пока нет
- Behcet S DiseaseДокумент34 страницыBehcet S DiseaseRendyОценок пока нет
- PiodermaДокумент43 страницыPiodermashlprtОценок пока нет
- Thacker - The Shadows of Atheology - Epidemics, Power and Life After FoucaultДокумент19 страницThacker - The Shadows of Atheology - Epidemics, Power and Life After FoucaultAmbaejo96Оценок пока нет
- Elektro Fisika Dan Sumber Fisis 1 Pertemuan 2Документ21 страницаElektro Fisika Dan Sumber Fisis 1 Pertemuan 2estherОценок пока нет
- Thyroid StormДокумент23 страницыThyroid Stormtogi_siahaanОценок пока нет
- Colibacillinum in Recurrent Cystitis: Case TwoДокумент1 страницаColibacillinum in Recurrent Cystitis: Case Twommalam1969Оценок пока нет
- Nailfold Capillaroscopy in Behçet's Disease, AnalysisДокумент3 страницыNailfold Capillaroscopy in Behçet's Disease, AnalysisAlinaBОценок пока нет
- Throat PowerpointДокумент29 страницThroat Powerpointminci sensei100% (8)
- DAFTAR PUSTAKAДокумент5 страницDAFTAR PUSTAKAWina BudiartiОценок пока нет
- ABDOMINAL PARACENTESIS PROCEDUREДокумент5 страницABDOMINAL PARACENTESIS PROCEDUREVijith.V.kumar100% (1)
- AMOEBIASISДокумент18 страницAMOEBIASISRosalie RosalesОценок пока нет
- Giardia lamblia in the Small IntestineДокумент16 страницGiardia lamblia in the Small IntestineRahul ChaudharyОценок пока нет
- Parasitology Guide Questions 1Документ2 страницыParasitology Guide Questions 1Cess LacatangoОценок пока нет
- CV Natalia SergeenkoДокумент4 страницыCV Natalia SergeenkoRobert BonomoОценок пока нет
- Reviewer in Grade 8 Mapeh Quarter 3Документ1 страницаReviewer in Grade 8 Mapeh Quarter 3Ruth Aramburo0% (1)
- A Novel Exercise For Improving Lower-Extremity Functional Fitness in The ElderlyДокумент7 страницA Novel Exercise For Improving Lower-Extremity Functional Fitness in The ElderlyJulia Dewi Eka GunawatiОценок пока нет
- @MedicalBooksStore 2012 (ERS Monograph) TuberculosisДокумент271 страница@MedicalBooksStore 2012 (ERS Monograph) TuberculosisHeri GunawanОценок пока нет