Вам также может понравиться
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (120)
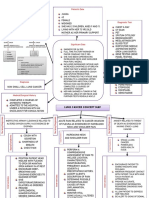
- Lung Cancer Concept Map-Group 2Документ2 страницыLung Cancer Concept Map-Group 2Maria Cristina100% (2)
- Cristian Colceriu - Elitele României - Prof. Dr. Ștefan Florian - Cluj Contemporary ElitesДокумент15 страницCristian Colceriu - Elitele României - Prof. Dr. Ștefan Florian - Cluj Contemporary Elitescristian colceriuОценок пока нет
- IGC 2 - Element 7 - Chemical HazardsДокумент67 страницIGC 2 - Element 7 - Chemical HazardsHim SiwakotiОценок пока нет
- Paediatric Question BankДокумент27 страницPaediatric Question BankBashiru SelemaniОценок пока нет
- Roles of Community Health NurseДокумент12 страницRoles of Community Health NurseEDz Delica SandovalОценок пока нет
- DH 220 - Specialty Office Visit - Teagan RubidaДокумент7 страницDH 220 - Specialty Office Visit - Teagan Rubidaapi-725916152Оценок пока нет
- Clinical PharmacokineticsДокумент31 страницаClinical PharmacokineticsArdiyanti Puspitasari100% (1)
- Legislator Email on Safe Patient HandlingДокумент5 страницLegislator Email on Safe Patient HandlingAnonymous dcpGmD60% (5)
- Diabetes Mellitus NCPДокумент6 страницDiabetes Mellitus NCPJOHN CARLO APATANОценок пока нет
- Aisha Gillan ResumeДокумент2 страницыAisha Gillan ResumeAisha GillanОценок пока нет
- Last Week DataДокумент15 страницLast Week Datajaswant0% (1)
- Wang 2016 JSES Trends Associated With Distal Biceps Tendon Repair in The U.S, 2007 To 2011Документ5 страницWang 2016 JSES Trends Associated With Distal Biceps Tendon Repair in The U.S, 2007 To 2011Kuozram No MasОценок пока нет
- OxfordДокумент3 страницыOxfordJaize Vyl RebutaОценок пока нет
- Jurnal ReadingДокумент13 страницJurnal Readingeliamegasari01Оценок пока нет
- Doctor'S Order Sheet: Mariano Marcos Memorial Hospital and Medical CenterДокумент1 страницаDoctor'S Order Sheet: Mariano Marcos Memorial Hospital and Medical CenterWyn Agustin100% (1)
- S4.M22.HO-Assessing Apical PulseДокумент2 страницыS4.M22.HO-Assessing Apical PulseNugraОценок пока нет
- Toward Nanotechnology-Enabled Approaches Against The COVID-19 PandemicДокумент24 страницыToward Nanotechnology-Enabled Approaches Against The COVID-19 Pandemicmadcraft9832Оценок пока нет
- Selective Grinding Goals and SequenceДокумент22 страницыSelective Grinding Goals and Sequencepaulina yañezОценок пока нет
- How To Observe and Assist in SurgeryДокумент33 страницыHow To Observe and Assist in SurgeryKareem Waleed Ibrahim HamimyОценок пока нет
- HsecpwpolicyДокумент93 страницыHsecpwpolicyapi-575088865Оценок пока нет
- Potent Antioxidant Acacia catechu ExtractДокумент1 страницаPotent Antioxidant Acacia catechu ExtractmdibashaОценок пока нет
- Icds N AayДокумент8 страницIcds N AayMeghan PaulОценок пока нет
- 7051N3M126Q411U7Документ69 страниц7051N3M126Q411U7naldihasibuanОценок пока нет
- 3 Triage DocumentationДокумент6 страниц3 Triage DocumentationKianne Rae Fernandez PalmaОценок пока нет
- Daftar Pustaka: Universitas Sumatera UtaraДокумент5 страницDaftar Pustaka: Universitas Sumatera UtaraNoona MuflihanaОценок пока нет
- Pediatrics Reviewer MCNДокумент17 страницPediatrics Reviewer MCNBrylee CudalОценок пока нет
- Dr. Prathap C Reddy, ChairmanДокумент3 страницыDr. Prathap C Reddy, ChairmansubhirockstarОценок пока нет
- Journal Maria F Delong - Impact of Plaque Burden Vs Stenosis On Ischemic Events in Patient With Coronary AtherosclerosisДокумент20 страницJournal Maria F Delong - Impact of Plaque Burden Vs Stenosis On Ischemic Events in Patient With Coronary AtherosclerosisAris MarutoОценок пока нет
- Who Pen 2020Документ85 страницWho Pen 2020Faye PalmaresОценок пока нет
- Micro para OSCE For YL6 BacteriaДокумент2 страницыMicro para OSCE For YL6 Bacteriagzldiwa100% (1)