Вам также может понравиться
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryОт EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryРейтинг: 3.5 из 5 звезд3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)От EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Рейтинг: 4.5 из 5 звезд4.5/5 (121)
- Never Split the Difference: Negotiating As If Your Life Depended On ItОт EverandNever Split the Difference: Negotiating As If Your Life Depended On ItРейтинг: 4.5 из 5 звезд4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingОт EverandThe Little Book of Hygge: Danish Secrets to Happy LivingРейтинг: 3.5 из 5 звезд3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaОт EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaРейтинг: 4.5 из 5 звезд4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeОт EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeРейтинг: 4 из 5 звезд4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreОт EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreРейтинг: 4 из 5 звезд4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyОт EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyРейтинг: 3.5 из 5 звезд3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersОт EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersРейтинг: 4.5 из 5 звезд4.5/5 (345)
- The Emperor of All Maladies: A Biography of CancerОт EverandThe Emperor of All Maladies: A Biography of CancerРейтинг: 4.5 из 5 звезд4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnОт EverandTeam of Rivals: The Political Genius of Abraham LincolnРейтинг: 4.5 из 5 звезд4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceОт EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceРейтинг: 4 из 5 звезд4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureОт EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureРейтинг: 4.5 из 5 звезд4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)От EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Рейтинг: 4 из 5 звезд4/5 (98)
- The Unwinding: An Inner History of the New AmericaОт EverandThe Unwinding: An Inner History of the New AmericaРейтинг: 4 из 5 звезд4/5 (45)
- Energy Audit Report by CPRIДокумент247 страницEnergy Audit Report by CPRImag_ktps20021520100% (2)
- Concrete Mix DesignДокумент11 страницConcrete Mix DesignV Vinoth Edac100% (1)
- 1.17 - Surreptitious Software Obfuscation, Watermarking, and Tamperproofing For Software ProtectionДокумент1 041 страница1.17 - Surreptitious Software Obfuscation, Watermarking, and Tamperproofing For Software ProtectionGabriel DiasОценок пока нет
- 5510 0004 04 - 18 1021 Basic Principles of Ship Propulsion - MAN PDFДокумент68 страниц5510 0004 04 - 18 1021 Basic Principles of Ship Propulsion - MAN PDFAlex FatecОценок пока нет
- EWAD-CF EEDEN15-435 Data Books EnglishДокумент42 страницыEWAD-CF EEDEN15-435 Data Books EnglishrpufitaОценок пока нет
- SAP QM Calibration MethodДокумент3 страницыSAP QM Calibration MethodvrkattulaОценок пока нет
- Mothballing Requires More Than Idle ThoughtДокумент4 страницыMothballing Requires More Than Idle Thoughtfawmer61Оценок пока нет
- 2016 FSAE Electric Vehicle Pedal Assembly DesignДокумент40 страниц2016 FSAE Electric Vehicle Pedal Assembly Designshubham rastogiОценок пока нет
- Yohimbine InjectionДокумент1 страницаYohimbine InjectionKasidit SornchaiОценок пока нет
- Cortec, VpCI-371 Application GuideДокумент2 страницыCortec, VpCI-371 Application Guidemonserrat PereaОценок пока нет
- Metron 05 CR DataДокумент10 страницMetron 05 CR DatamkgohОценок пока нет
- Introduction To Research MethodsДокумент11 страницIntroduction To Research MethodsKamlakar SadavarteОценок пока нет
- FELPRO - Tablas-de-Torque - 035Документ1 страницаFELPRO - Tablas-de-Torque - 035Clodoaldo BiassioОценок пока нет
- OL ICT First Term Kengalla Maha Vidyalaya English Medium Grade 11 MCQ Paper 2019Документ5 страницOL ICT First Term Kengalla Maha Vidyalaya English Medium Grade 11 MCQ Paper 2019mazhus123Оценок пока нет
- Lab 4 SpectrophotometryДокумент6 страницLab 4 SpectrophotometryCheng FuОценок пока нет
- DefaultДокумент49 страницDefaultmaruka33100% (1)
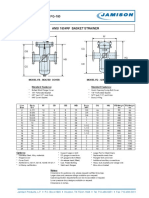
- FB-150 FQ-150 Basket StrainerДокумент1 страницаFB-150 FQ-150 Basket Strainerklich77Оценок пока нет
- Code Division DuplexingДокумент19 страницCode Division DuplexingNitin SakpalОценок пока нет
- Cobol Language Fundamentals: Structured COBOL Programming, Stern & Stern, 9th Ed ItionДокумент53 страницыCobol Language Fundamentals: Structured COBOL Programming, Stern & Stern, 9th Ed ItionAsk NameОценок пока нет
- Viscosity Measurements On Oligoesters From Terephthalic Acid and GlycoДокумент7 страницViscosity Measurements On Oligoesters From Terephthalic Acid and GlycoMaria RincondeОценок пока нет
- Standard Test Method For Density and Void Content of Freshly Mixed Pervious ConcreteДокумент4 страницыStandard Test Method For Density and Void Content of Freshly Mixed Pervious ConcreteManaswini VadlamaniОценок пока нет
- Clipping Clamping CircuitsДокумент7 страницClipping Clamping CircuitsPavan SaiОценок пока нет
- Alarm ListДокумент4 страницыAlarm ListMirela Perenda ŠabićОценок пока нет
- Laser in ProsthodonticsДокумент84 страницыLaser in ProsthodonticsmarwaОценок пока нет
- EARTH AND LIFE SCIENCE II Answer KeyДокумент4 страницыEARTH AND LIFE SCIENCE II Answer Keyjelena jorgeoОценок пока нет
- Codigo Ficheros PHPДокумент33 страницыCodigo Ficheros PHPm_montielОценок пока нет
- Vector AlgebraДокумент7 страницVector AlgebraDeeeОценок пока нет
- Part 1Документ120 страницPart 1Raju Halder0% (1)
- Clase 13-06Документ28 страницClase 13-06Jhurema NihuaОценок пока нет
- Atmos S 351 - Service ManualДокумент40 страницAtmos S 351 - Service ManualcuetlaxochitlОценок пока нет