Вам также может понравиться
- s12888 019 2350 XДокумент10 страницs12888 019 2350 XTrần Thanh KhiếtОценок пока нет
- Efficacy of Interventions Based On The Use of Information and Communication Technologies For The Promotion of Active AgingДокумент11 страницEfficacy of Interventions Based On The Use of Information and Communication Technologies For The Promotion of Active AgingAlvaro Astasio PicadoОценок пока нет
- Comparison of Mobile Health Technology Use For Self-Tracking Between Older Adults and The General Adult Population in Canada: Cross-Sectional SurveyДокумент14 страницComparison of Mobile Health Technology Use For Self-Tracking Between Older Adults and The General Adult Population in Canada: Cross-Sectional Surveyerpriya2023Оценок пока нет
- Mhealth Adoption Among Older Chinese Adults A Conceptual Model With Design Suggestions - 2023 - Taylor and Francis LTDДокумент13 страницMhealth Adoption Among Older Chinese Adults A Conceptual Model With Design Suggestions - 2023 - Taylor and Francis LTDAli AhmedОценок пока нет
- WhenДокумент7 страницWhenjames thottanОценок пока нет
- The Smartphone in Medicine AДокумент15 страницThe Smartphone in Medicine Arichardong lauОценок пока нет
- Mobile Phone Use: Linking Physics Knowledge and Health AwarenessДокумент10 страницMobile Phone Use: Linking Physics Knowledge and Health AwarenessPsychology and Education: A Multidisciplinary JournalОценок пока нет
- Mobile Technologies and Healthy Ageing A Bibliometric Analysis On Publication Trends and Knowledge Structure of MHealth Research For Older AdultsДокумент14 страницMobile Technologies and Healthy Ageing A Bibliometric Analysis On Publication Trends and Knowledge Structure of MHealth Research For Older Adultstri lestariОценок пока нет
- Behaviour Change Communication in Health PromotionДокумент11 страницBehaviour Change Communication in Health Promotionsandranahdar611Оценок пока нет
- Behaviour Change Communication in Health Promotion: Appropriate Practices and Promising ApproachesДокумент11 страницBehaviour Change Communication in Health Promotion: Appropriate Practices and Promising ApproachesWasihun AbduОценок пока нет
- COVID-19 Tech Use by PH YouthДокумент5 страницCOVID-19 Tech Use by PH YouthAlexxa Gabrielle JaneoОценок пока нет
- A Usability Evaluation Instrument For Pain Management Mobile Applications An Elderly S PerspectiveДокумент18 страницA Usability Evaluation Instrument For Pain Management Mobile Applications An Elderly S Perspectiveummemariyashah526Оценок пока нет
- Mhealth: Mobile Technology Poised To Enable A New Era in Health CareДокумент54 страницыMhealth: Mobile Technology Poised To Enable A New Era in Health CaremhemaraОценок пока нет
- Journal of Biomedical Informatics: Predrag Klasnja, Wanda PrattДокумент15 страницJournal of Biomedical Informatics: Predrag Klasnja, Wanda PrattSteveEpsteinОценок пока нет
- Antecedents and Consequences of Problematic Smartphone Use++++LitertureДокумент47 страницAntecedents and Consequences of Problematic Smartphone Use++++LitertureZaid MarwanОценок пока нет
- Strategies for Successful mHealth Research Based on Lessons from 3 Mobile Intervention StudiesДокумент11 страницStrategies for Successful mHealth Research Based on Lessons from 3 Mobile Intervention StudiesNadhilaОценок пока нет
- Using E-Technologies in Clinical Trials Rosa 2015Документ14 страницUsing E-Technologies in Clinical Trials Rosa 2015Itzcoatl Torres AlcantaraОценок пока нет
- Health and Fitness Apps: A Bibliometric Analysis Focusing On The Increased Usage During and After Covid-19Документ17 страницHealth and Fitness Apps: A Bibliometric Analysis Focusing On The Increased Usage During and After Covid-19sunilbiwal020Оценок пока нет
- MDIwMTMxODU2 PDFДокумент8 страницMDIwMTMxODU2 PDFPriyanjali SainiОценок пока нет
- Review of Researches On Smartphone Applications For Physical Activity Promotion in Healthy AdultsДокумент9 страницReview of Researches On Smartphone Applications For Physical Activity Promotion in Healthy AdultsJorge MariaОценок пока нет
- FC Xsltgalley 2661 32465 11 PBДокумент11 страницFC Xsltgalley 2661 32465 11 PBRob Sandoval StebanОценок пока нет
- Research Ethics For Mobile Sensing Device Use by Vulnerable PopulationsДокумент8 страницResearch Ethics For Mobile Sensing Device Use by Vulnerable PopulationsAndreea MadalinaОценок пока нет
- Women Using Digital Technology As A Source For Health Seeking Information: A Short Study in MeghalayaДокумент16 страницWomen Using Digital Technology As A Source For Health Seeking Information: A Short Study in MeghalayaImpact JournalsОценок пока нет
- A Study On Some of The Common Health Effects of Cell-Phones Amongst College Students PDFДокумент4 страницыA Study On Some of The Common Health Effects of Cell-Phones Amongst College Students PDFSii JiingОценок пока нет
- Trends in Healthcare and Medical InnovationДокумент7 страницTrends in Healthcare and Medical InnovationThe Brown Bag Gang100% (1)
- Artikel KualitativeДокумент12 страницArtikel KualitativeRiski DpОценок пока нет
- 81-Article Text-153-1-10-20210705Документ25 страниц81-Article Text-153-1-10-20210705edyОценок пока нет
- Neck Pain 6.ms - IdДокумент8 страницNeck Pain 6.ms - Idwhoaa ckckОценок пока нет
- Sustainability 08 00466Документ16 страницSustainability 08 00466Amgad RedaОценок пока нет
- Design Principles For Health WearablesДокумент11 страницDesign Principles For Health WearablesIgnacio NolascoОценок пока нет
- Impact of Digital Media On Sleep Pattern Disturbance in Medical and Nursing StudentsДокумент7 страницImpact of Digital Media On Sleep Pattern Disturbance in Medical and Nursing StudentsValarmathiОценок пока нет
- Older adults talk technology: Technology usage and attitudesДокумент12 страницOlder adults talk technology: Technology usage and attitudesJuliana GomesОценок пока нет
- Ethical Issues of Social Media Usage in HealthcareДокумент12 страницEthical Issues of Social Media Usage in HealthcareFreddy ChopperxОценок пока нет
- Impact of Mobile Phone Usage On Some Health Aspects of Children and Adolescents: Evidence Based Review ArticleДокумент3 страницыImpact of Mobile Phone Usage On Some Health Aspects of Children and Adolescents: Evidence Based Review ArticlebillОценок пока нет
- 1.global Overview of Mobile Technology in The Area of Chronic Disease ManagementДокумент5 страниц1.global Overview of Mobile Technology in The Area of Chronic Disease Managementbankhouse2023Оценок пока нет
- Impact of Mobile Phone Addiction On Adolescent's Life: A Literature ReviewДокумент6 страницImpact of Mobile Phone Addiction On Adolescent's Life: A Literature ReviewJohn Philip VillanuevaОценок пока нет
- Android Based Health Management App Monitors MedicationДокумент43 страницыAndroid Based Health Management App Monitors MedicationDaryll TorresОценок пока нет
- DigitalMedia BasedNutritionHealthCommunicationModelДокумент6 страницDigitalMedia BasedNutritionHealthCommunicationModelHaris Prayudi -Оценок пока нет
- Ji 5Документ16 страницJi 5Hijrawati IrhaeОценок пока нет
- Maria Renata Guarneri, Roberto Sironi and Paolo Perego: Mariarenata - Guarneri@polimi - ItДокумент4 страницыMaria Renata Guarneri, Roberto Sironi and Paolo Perego: Mariarenata - Guarneri@polimi - ItAnkit VermaОценок пока нет
- IJMPR0101002Документ14 страницIJMPR0101002IJMPR JournalОценок пока нет
- Literature Review On Monitoring Technologies andДокумент25 страницLiterature Review On Monitoring Technologies andOnur OzdemirОценок пока нет
- Nudge SmartphoneДокумент48 страницNudge SmartphoneAvaniОценок пока нет
- A Survey On Ambient-Assisted Living Tools For Older AdultsДокумент12 страницA Survey On Ambient-Assisted Living Tools For Older AdultsOnur Ozdemir0% (1)
- Capstone HuacasiДокумент40 страницCapstone Huacasiapi-397532577Оценок пока нет
- How Smartphones Are Changing The Face of Mobile and Participatory Healthcare: An Overview, With Example From eCAALYXДокумент14 страницHow Smartphones Are Changing The Face of Mobile and Participatory Healthcare: An Overview, With Example From eCAALYXPrasitha MОценок пока нет
- Jayanti EtalДокумент7 страницJayanti EtaleditorijmrhsОценок пока нет
- Effectiveness of Personal Health Monitoring through Mobile TechnologiesДокумент9 страницEffectiveness of Personal Health Monitoring through Mobile TechnologiesGloria Marisse BaclayОценок пока нет
- Team Project 3Документ6 страницTeam Project 3api-638721920Оценок пока нет
- Silva 2015Документ8 страницSilva 2015Abdul QodirОценок пока нет
- Art. 2 DoneДокумент12 страницArt. 2 DoneGustavo GarciaОценок пока нет
- Inter - Untuk Melihat Sejauh Mana Pengaruh Apk Mhealth Dalam Mengelola Obesitas Dan Manaj Diri Pada Pasien DMДокумент14 страницInter - Untuk Melihat Sejauh Mana Pengaruh Apk Mhealth Dalam Mengelola Obesitas Dan Manaj Diri Pada Pasien DMGladis IsmailОценок пока нет
- Using Smart Speaker Technology For Health and Well-Being in An Older Adult Population: Pre-Post Feasibility StudyДокумент11 страницUsing Smart Speaker Technology For Health and Well-Being in An Older Adult Population: Pre-Post Feasibility StudyTony MallorcaОценок пока нет
- Smart Hospital System Using Android With Facilities of Smart Ambulance Patient Assist Live Patient Status Medical Requirement AlertДокумент15 страницSmart Hospital System Using Android With Facilities of Smart Ambulance Patient Assist Live Patient Status Medical Requirement AlertDhanashree ChaudhariОценок пока нет
- CDC Mhealth For Aging Adults 11 - 0241Документ4 страницыCDC Mhealth For Aging Adults 11 - 0241kmmhealyОценок пока нет
- HayesCAREER SharedДокумент24 страницыHayesCAREER SharedZhongxing YuОценок пока нет
- Mobile Phone Technology in Chronic Disease Management: Art ScienceДокумент4 страницыMobile Phone Technology in Chronic Disease Management: Art Scienceinnani wildaniaОценок пока нет
- Taxonomy of mHealth applicationsДокумент10 страницTaxonomy of mHealth applicationsBrhayan Elias Periñan RuizОценок пока нет
- IndianJCommunityMed393178-162667 043106Документ5 страницIndianJCommunityMed393178-162667 043106Community MedicineОценок пока нет
- Developing Medical Apps and mHealth Interventions: A Guide for Researchers, Physicians and InformaticiansОт EverandDeveloping Medical Apps and mHealth Interventions: A Guide for Researchers, Physicians and InformaticiansОценок пока нет
- A Proposal For Monitoring Patients With Heart Failure Via "Smart Phone Technology "-Based ElectrocardiogramsДокумент8 страницA Proposal For Monitoring Patients With Heart Failure Via "Smart Phone Technology "-Based ElectrocardiogramsGabriella CsernákОценок пока нет
- Surface 12 Lead Electrocardiogram Recordings Using Smart Phone TechnologyДокумент7 страницSurface 12 Lead Electrocardiogram Recordings Using Smart Phone TechnologyGabriella CsernákОценок пока нет
- Electrophysiologic findings in ventricular noncompactionДокумент2 страницыElectrophysiologic findings in ventricular noncompactionGabriella CsernákОценок пока нет
- The Influence of The Children's Inner Health Picture OnДокумент4 страницыThe Influence of The Children's Inner Health Picture OnGabriella CsernákОценок пока нет
- 2021 Ishne/Hrs/Ehra/Aphrs Collaborative Statement On Mhealth in Arrhythmia Management: Digital Medical Tools For Heart Rhythm ProfessionalsДокумент51 страница2021 Ishne/Hrs/Ehra/Aphrs Collaborative Statement On Mhealth in Arrhythmia Management: Digital Medical Tools For Heart Rhythm ProfessionalsGabriella CsernákОценок пока нет
- Analysis and Postprocessing of ECG or Heart Rate Data From Wearable Devices Beyond The Proprietary Cloud and App Infrastructure of The VendorsДокумент8 страницAnalysis and Postprocessing of ECG or Heart Rate Data From Wearable Devices Beyond The Proprietary Cloud and App Infrastructure of The VendorsGabriella CsernákОценок пока нет
- Wearing Your Heart On Your WristДокумент3 страницыWearing Your Heart On Your WristGabriella CsernákОценок пока нет
- The Contribution of Organised Sports To Physical Activity IДокумент6 страницThe Contribution of Organised Sports To Physical Activity IGabriella CsernákОценок пока нет
- Atrial Chamber Remodelling in Healthy PDFДокумент6 страницAtrial Chamber Remodelling in Healthy PDFGabriella CsernákОценок пока нет
- Author 'S Accepted Manuscript: 10.1016/j.hrthm.2016.02.006Документ25 страницAuthor 'S Accepted Manuscript: 10.1016/j.hrthm.2016.02.006Gabriella CsernákОценок пока нет
- Training-Induced Right Ventricular Remodelling in Pre-AdolescДокумент6 страницTraining-Induced Right Ventricular Remodelling in Pre-AdolescGabriella CsernákОценок пока нет
- (2013) Children's Heart Rate Variability As Stress Indicator Association With PDFДокумент8 страниц(2013) Children's Heart Rate Variability As Stress Indicator Association With PDFGabriella CsernákОценок пока нет
- Resting High Frequency Heart Rate Variability SelectivДокумент12 страницResting High Frequency Heart Rate Variability SelectivGabriella CsernákОценок пока нет
- 1 s2.0 S1109966618304974 MainДокумент7 страниц1 s2.0 S1109966618304974 MainhabibiОценок пока нет
- Smartphone-Enabled Pulse Rate Variability An Alternative Methodology FДокумент8 страницSmartphone-Enabled Pulse Rate Variability An Alternative Methodology FGabriella CsernákОценок пока нет
- 1 s2.0 S1875952115000166 Main PDFДокумент11 страниц1 s2.0 S1875952115000166 Main PDFGabriella CsernákОценок пока нет
- Physical Activity Is Associated With Better Vascular Function in Children andДокумент27 страницPhysical Activity Is Associated With Better Vascular Function in Children andGabriella CsernákОценок пока нет
- Analyses of Heart Rate Variability in Young PDFДокумент5 страницAnalyses of Heart Rate Variability in Young PDFGabriella CsernákОценок пока нет
- 1 s2.0 S0921889016303268 MainДокумент10 страниц1 s2.0 S0921889016303268 MainGabriella CsernákОценок пока нет
- Meta Análisis Variabilidad de Frecuencia CardíacaДокумент10 страницMeta Análisis Variabilidad de Frecuencia CardíacaVicente GaticaОценок пока нет
- 1 s2.0 S1877705812026094 Main PDFДокумент9 страниц1 s2.0 S1877705812026094 Main PDFGabriella CsernákОценок пока нет
- 1 s2.0 S1474442216301260 Main PDFДокумент2 страницы1 s2.0 S1474442216301260 Main PDFGabriella CsernákОценок пока нет
- 1 s2.0 S0161475416302457 MainДокумент10 страниц1 s2.0 S0161475416302457 MainGabriella CsernákОценок пока нет
- 1 s2.0 S1877050915036947 MainДокумент8 страниц1 s2.0 S1877050915036947 MainGabriella CsernákОценок пока нет
- 1 s2.0 S1319157815000154 Main PDFДокумент10 страниц1 s2.0 S1319157815000154 Main PDFGabriella CsernákОценок пока нет
- 1 s2.0 S1350453318300432 Main PDFДокумент9 страниц1 s2.0 S1350453318300432 Main PDFGabriella CsernákОценок пока нет
- 1 s2.0 S1052305717304378 Main PDFДокумент8 страниц1 s2.0 S1052305717304378 Main PDFGabriella CsernákОценок пока нет
- 1 s2.0 S2211285518302878 MainДокумент9 страниц1 s2.0 S2211285518302878 MainGabriella CsernákОценок пока нет
- 1 s2.0 S105230571630307X MainДокумент7 страниц1 s2.0 S105230571630307X MainGabriella CsernákОценок пока нет
- 1 s2.0 S1877050915036947 MainДокумент8 страниц1 s2.0 S1877050915036947 MainGabriella CsernákОценок пока нет
- May 17, 2013 Strathmore TimesДокумент36 страницMay 17, 2013 Strathmore TimesStrathmore TimesОценок пока нет
- PicДокумент815 страницPicSiva PratapОценок пока нет
- Listening Comprehension SkillsДокумент2 страницыListening Comprehension SkillsAngela Widya RОценок пока нет
- Chapter 05: Selecting The Ventilator and The ModeДокумент13 страницChapter 05: Selecting The Ventilator and The Modespace100% (1)
- Pursed Lip BreathingДокумент4 страницыPursed Lip BreathingDinesh KumarОценок пока нет
- Anti AcidsДокумент29 страницAnti AcidsUtkarsh RaizadaОценок пока нет
- Fascia - East and WestДокумент3 страницыFascia - East and Westwalterego58Оценок пока нет
- Teen Depression TP UwrtДокумент5 страницTeen Depression TP Uwrtapi-338204602Оценок пока нет
- 10 11648 J SJPH S 2015030501 21Документ6 страниц10 11648 J SJPH S 2015030501 21Muhammad FakhriОценок пока нет
- Eu Yan Sang 9-29-09Документ19 страницEu Yan Sang 9-29-09putsadinОценок пока нет
- Murmur: CausesДокумент21 страницаMurmur: CausesJessica AdhykaОценок пока нет
- SOTAH CourseGuideДокумент198 страницSOTAH CourseGuideDee100% (1)
- Asia Pacific Obesity 2000Документ56 страницAsia Pacific Obesity 2000Melissa SindiongОценок пока нет
- What Is Homeopathy - Homeopathic Medicine - HomeopathyДокумент5 страницWhat Is Homeopathy - Homeopathic Medicine - HomeopathyHilion FLAVIOОценок пока нет
- Se SN AspirinДокумент5 страницSe SN Aspirinnguyen thu trangОценок пока нет
- Formularium Rs Claire Medika DraftДокумент111 страницFormularium Rs Claire Medika DraftSuhita TuloyОценок пока нет
- Capstone 1-3 For DefenseДокумент27 страницCapstone 1-3 For DefenseRussel AloceljaОценок пока нет
- Emotions, Stress, and HealthДокумент57 страницEmotions, Stress, and HealthNadwa NasirОценок пока нет
- Trusted Medical Answers-In Seconds.: Lipid DisordersДокумент13 страницTrusted Medical Answers-In Seconds.: Lipid DisordersMohammed shamiul Shahid100% (1)
- BPJS Rawat Inap Kelas II Januari 2016Документ65 страницBPJS Rawat Inap Kelas II Januari 2016fitriОценок пока нет
- Hot Sitz BathДокумент12 страницHot Sitz BathJosiah VillacampaОценок пока нет
- A Study On Kashmiri Cuisine Wazwan: M.B.B.S, Toronto, On Bagatparrayporaumer Enclave H.No 21 Srinagar, Kashmir.19005Документ8 страницA Study On Kashmiri Cuisine Wazwan: M.B.B.S, Toronto, On Bagatparrayporaumer Enclave H.No 21 Srinagar, Kashmir.19005Usama ButtОценок пока нет
- IMP Malay Kumar Ganguly v. Dr. Sukumar Mukherjee, (SC) Law Finder Doc Id # 202541Документ94 страницыIMP Malay Kumar Ganguly v. Dr. Sukumar Mukherjee, (SC) Law Finder Doc Id # 202541Arihant RoyОценок пока нет
- Quiz PeriДокумент3 страницыQuiz PeriAlina Juliana MagopetОценок пока нет
- Cultural Competence in HealthcareДокумент26 страницCultural Competence in HealthcareNestor BalboaОценок пока нет
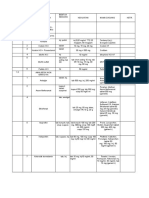
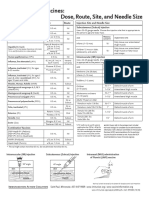
- Injection Site and Needle Size Vaccine Dose RouteДокумент1 страницаInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaОценок пока нет
- DBT in BPD Case PresentationДокумент105 страницDBT in BPD Case PresentationPrasanta Roy100% (1)
- Nidhi Meditech Systems Gujarat IndiaДокумент10 страницNidhi Meditech Systems Gujarat IndiaNidhi Meditech SystemsОценок пока нет
- Medical Terminology Ar and Eng PDFДокумент18 страницMedical Terminology Ar and Eng PDFRead me100% (1)
- Document 20Документ5 страницDocument 20Laura FreemanОценок пока нет